Downloaded 23 times

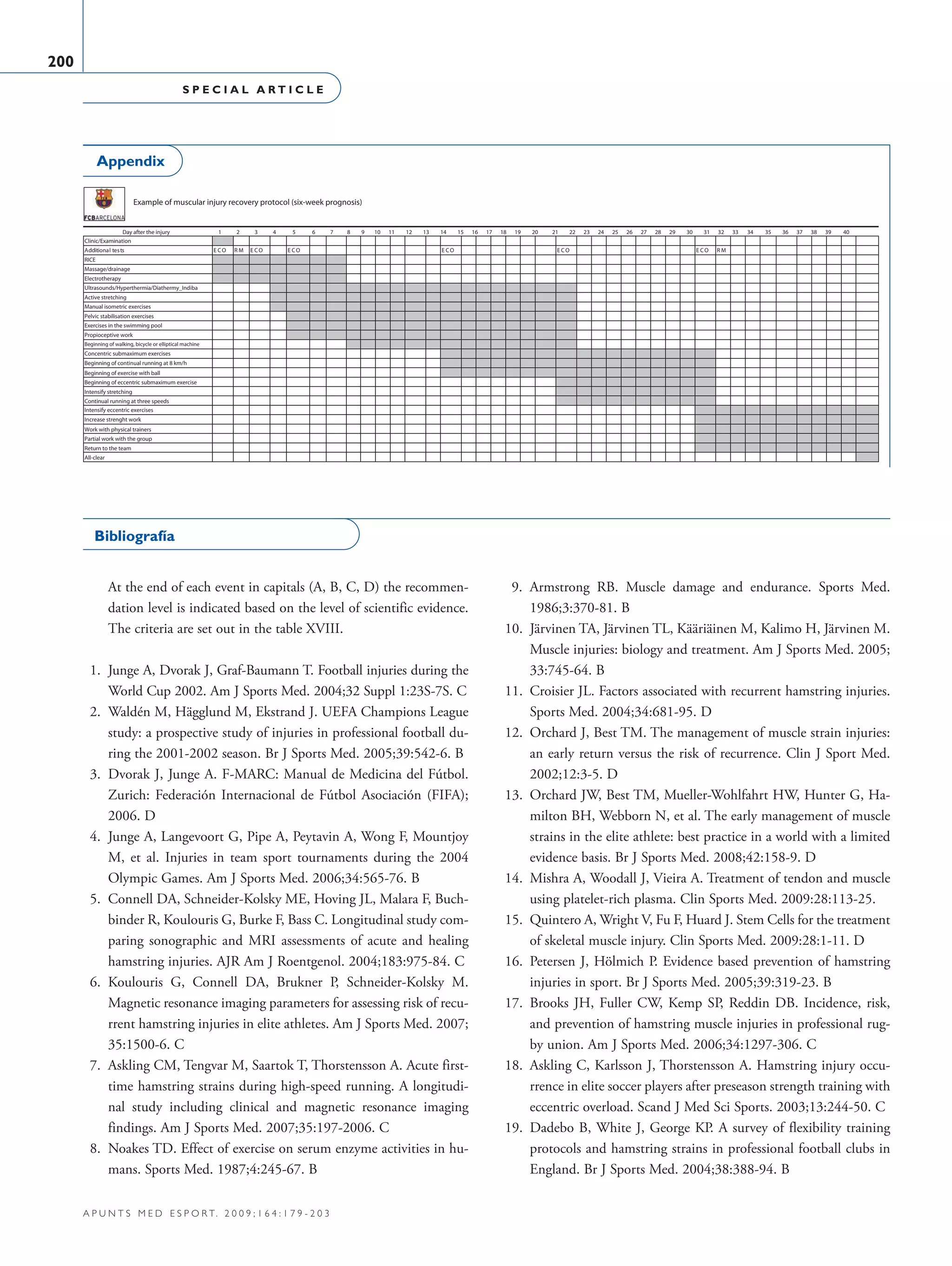
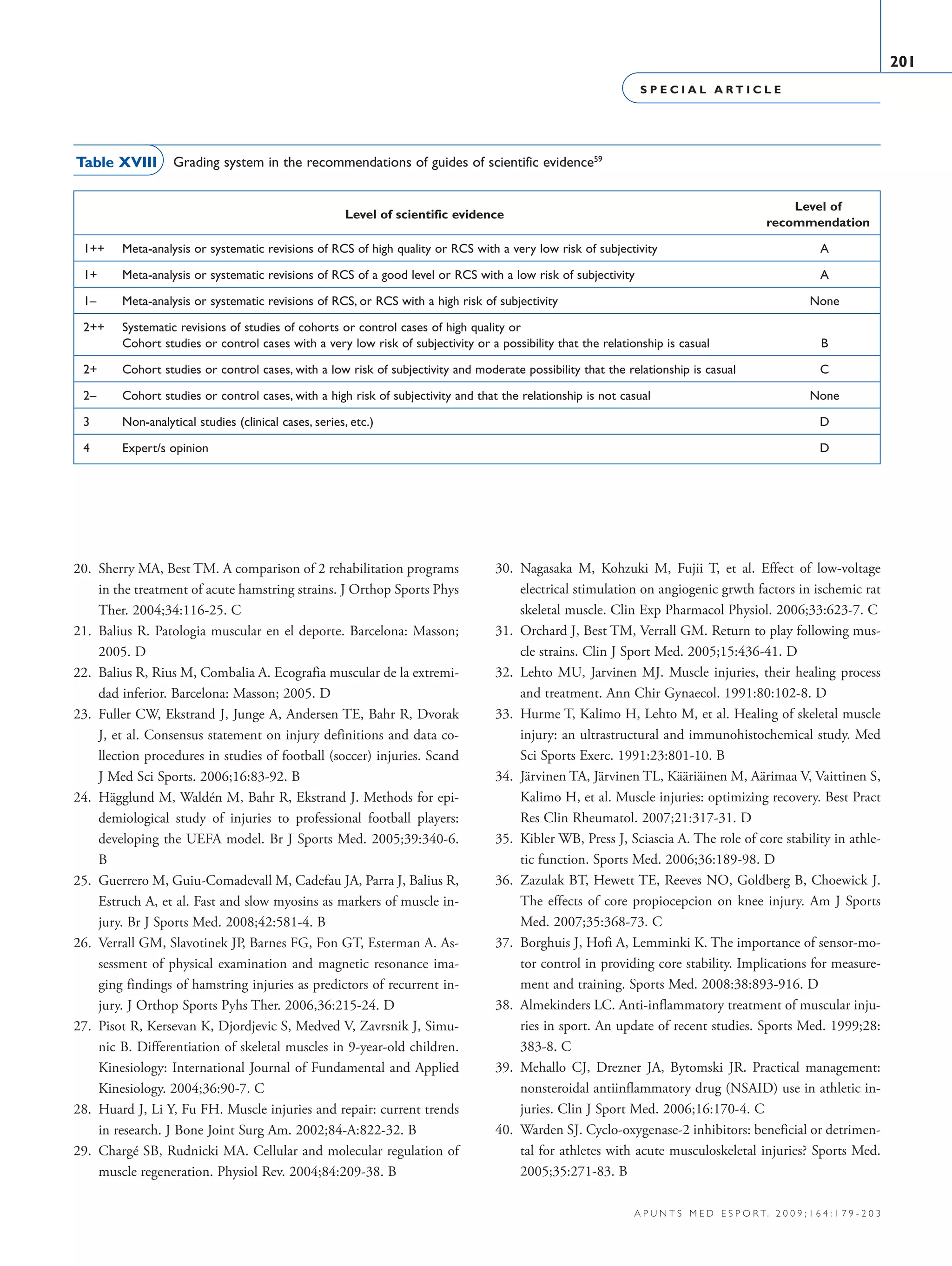

This document serves as a clinical practice guide for muscular injuries in football, detailing their epidemiology, diagnosis, treatment, and prevention strategies. It highlights the high incidence of muscular injuries in professional sports, particularly football, and gives insight into diagnosis methods, treatment protocols, and preventive measures based on current research. The aim is to provide clear and practical guidelines for managing muscular injuries among players of FC Barcelona, drawing on data and studies over several seasons.







































































