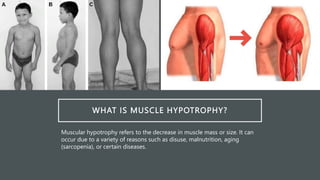
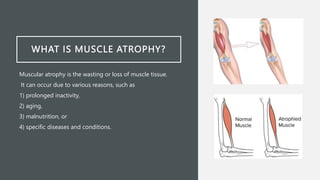
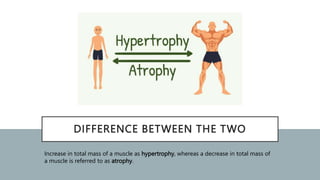
Muscle hypotrophy and atrophy refer to decreases in muscle mass. Hypotrophy is a decrease in size, while atrophy is a loss of muscle tissue. Atrophy can result from inactivity, aging, malnutrition or disease. Diagnosis involves medical history, exams, and tests like blood tests, imaging, and biopsies. Treatment focuses on exercise, nutrition, physical therapy, and treating any underlying causes. Case studies showed how genetic disorders can cause unusual hypotrophy or neurological disorders can lead to progressive atrophy.