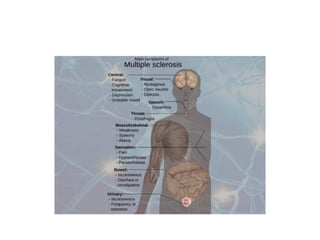
Multiple sclerosis is a chronic neurological disorder that affects the central nervous system. It is characterized by lesions in the brain and spinal cord that cause inflammation and damage to the myelin sheath surrounding nerves. Symptoms vary depending on the location of lesions but can include visual disturbances, limb weakness, and sensory issues. The course of the disease is usually relapsing-remitting, with periods of symptoms followed by remission, though it can also be progressive with steady worsening over time. While its exact causes are unknown, it is thought to involve an environmental trigger in genetically susceptible individuals. Treatment focuses on managing relapses, symptoms, and slowing disease progression using medications.