Plasma Cells
Dyscrasias/Paraproteinaemias
• Heterogeneousgroup of disorders characterised by deranged
proliferation of a single clone of plasma cells or B lymphocytes
and usually associated with detectable monoclonal
immunoglobulin (paraprotein or M-protein) in serum and/or
urine.
They are invariably fatal chronic clonal B cell malignancy
characterised by a progressive clinical course lasting some 3–
6.5 yr from diagnosis
In the USA, the estimated 5-year survival rate is about 40%
Survival is higher in younger patients than in the elderly
3
4.
Introduction
• They aregenerally characterised by:
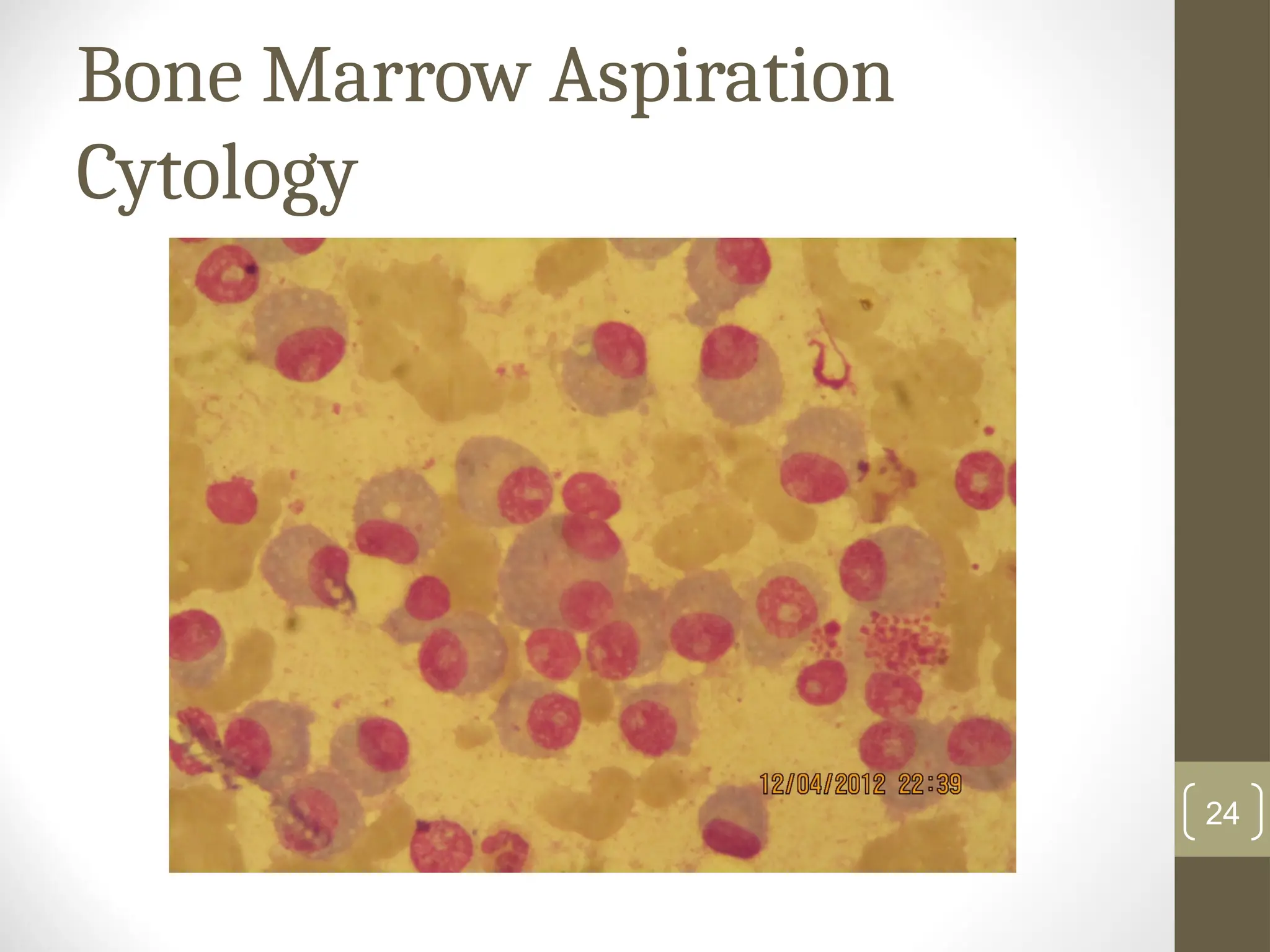
• proliferation of clonal neoplastic plasma cells in the bone marrow,
and sometimes in the extramedullary tissues.
• synthesis of immunologically incompetent myeloma (M-) or
paraproteins (with identical heavy chain and light chain) into the
serum and/or urine resulting in renal failure and bone
disease (pathological fractures, wedge compression
fracture of the vertebrae & cord compression spinal)
• Suppression of normal Ig production and high susceptibility of
patients to chronic bacterial infections including encapsulated
organisms: S. pneumoniae, H.influenzae and N. meningitides
4
5.
Pathogenesis
• Plasma cellsare terminally differentiated B- lymphocytes that
secret antibodies.
• In immunocompetent individuals, antibody synthesis and B-
cell proliferation are tightly controlled.
• The control is lost when there is a genetic accident due to
translocation of a promoter gene to another chromosome
where it stimulates an antibody gene to overproduction.
• Such genetic accidents eventually lead to malignant
transformation and development of malignancies as in
myeloma
5
6.
Pathogenesis contnd
Pathogenetically,myeloma arises from a primary chromosomal
translocation between the immunoglobulin heavy chain (IgH)
gene on chromosome 14 (locus q32) and an oncogene (more
often: 11q13, 6p21, 4p16 & 16q23).
The mutation causes dysregulation of the oncogene, with
resultant malignant transformation and development of
multiple myeloma.
6
7.
Pathogenesis contnd
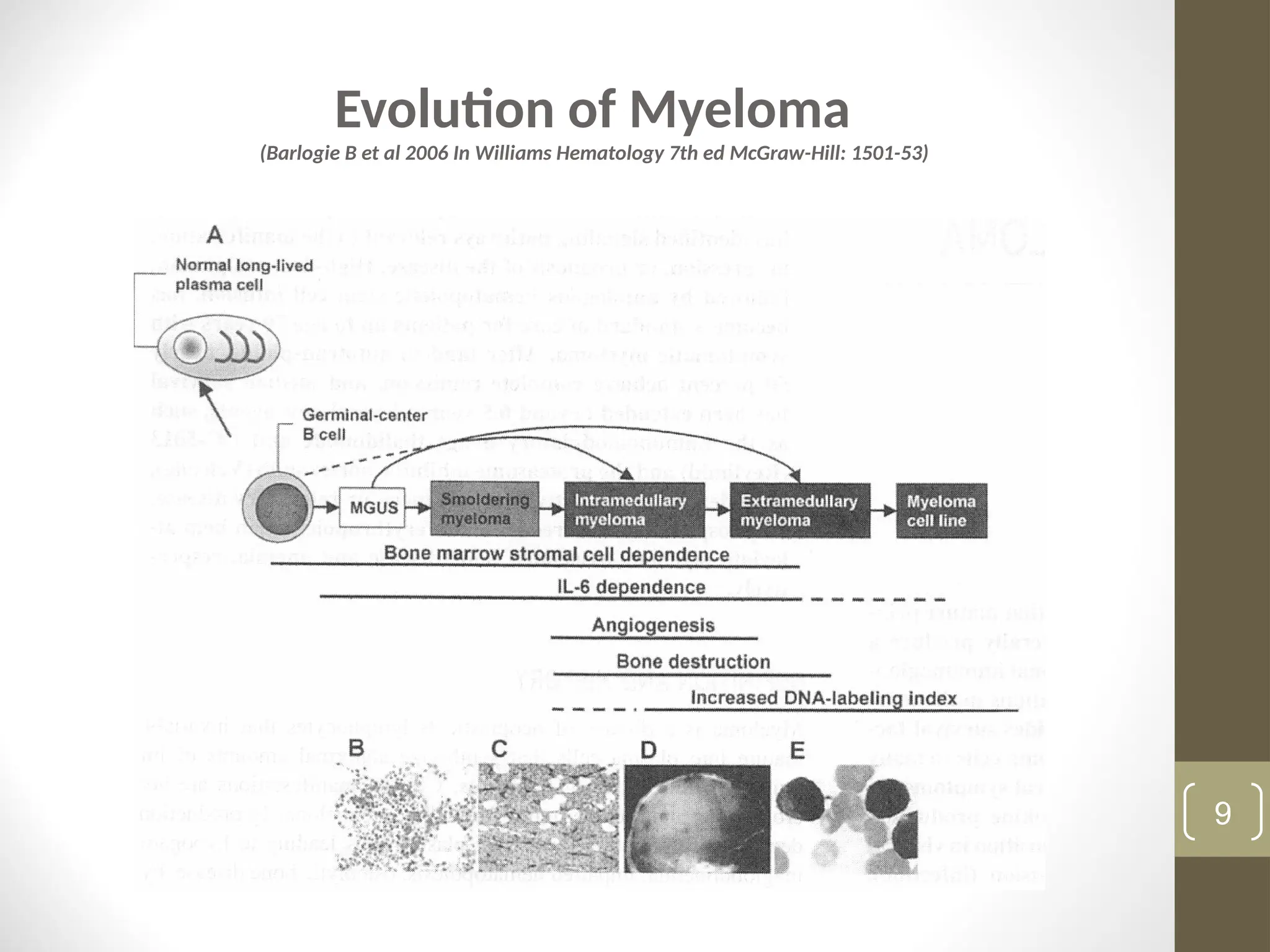
Adhesionof myeloma cells to bone marrow stromal cells
induces the cells to secret osteoclast-activating factors such as
interleukin IL-6, IL-1β, TNF-β and RANK-ligand that are
responsible for the myeloma related end organ damage and
tissue impairment.
The microenvironment created by the cytokines also enhances
angiogenesis, which allows the malignant plasma cells thrive
The antibodies (paraproteins) produced by the malignant
clonal plasma cells are deposited in various organs, leading to
renal failure, polyneuropathy and various other myeloma-
associated symptoms
7
8.
Pathogenesis contnd
• BMinfiltration causes anaemia.
• Suppression of normal Ig production predisposes to infection.
• Physicochemical properties of paraprotein determine amyloid
deposition, renal damage and hyperviscosity (IgA and IgG).
Classification of PlasmaCell Neoplasms
Multiple myeloma (myelomatosis)
Monoclonal gammopathy of undetermined significance
(MGUS)
Smouldering myeloma (about 20% of plasma cell tumours):
monoclonal gammopathy with atypical plasma cells in the
bone marrow, but without anaemia, bone diseases, or renal
failure.
Solitary plasmacytoma of bone: localised single tumour of
bones such as the vertebral column, pelvis, femur or the
humerus; marrow not diagnostic of myeloma; normal skeletal
survey; absence of end organ damage; absent or minimal M-
protein in serum and/or urine. Progression to myeloma occurs
in 50% of patients within 3-4 yrs, 10-yr disease-free survival is
25-40%; local radiotherapy is curative 10
11.
Classification of PlasmaCell Neoplasms
Extramedullary plasmacytoma: single localised soft tissue
plasma cell tumour of any of the upper respiratory tract,
gastrointestinal tract (stomach, rectum), skin, prostate and
retroperitoneum. Bone marrow, skeletal survey and end organ
are normal, serum and urinary paraproteins are undetectable
or just minimal. Predominance of IgA monoclonal protein.
Radiotherapy is curative and progression to myeloma in 15% of
patients. (Kyle RA, et al. Br J Haematol 2003; 121: 749–757)
Multiple solitary plasmacytomas: uncommon, monoclonal
protein rarely seen in serum and/or urine; multiple localized
areas of bone destruction or extramedullary plasma cell
tumours that may be recurrent; marrow & skeletal survey
essentially normal; end organ damage is absent. Recurrent
disease is treated as for myeloma with radiation and
chemotherapy.
11
12.
Classification of PlasmaCell Neoplasms
Plasma cell leukaemia: bone marrow plasmacytosis with
circulating plasma cells of at least 2 x 10^9/L, or plasma cells >
20% of circulating leucocytes. Response to conventional
therapy is very poor, stem cell transplantation is promising
(Drake, MB, et al. Haematologica 2010; 95: 804-9)
Lymphoplasmacytic lymphoma (eg, Waldenstrom’s
macroglobulinaemia)
Heavy chain disease
Multiple myeloma is the commonest of the neoplasms and
would be the subject of subsequent discuss
12
13.
Multiple Myeloma
• Themajority of cases of myeloma
present de novo but some cases are
preceded by asymptomatic
monoclonal gammopathy of
undetermined significance(MGUS)
13
14.
Myeloma Sub-Types
IgGmyeloma 60-70%
IgA 25-30%
IgD 1-2%
IgE and IgM < 1% (very rare)
*Light chain myeloma 15-25%
**Non-Secretory myeloma 1-3%
(absence of paraprotein in serum and/or urine; marrow clonal
plasmacytosis ≥ 10% or plasmacytoma; presence of myeloma
related organ or tissue impairment including bone lesions)
* Synthesis of only or light chain paraprotein, exreted as Bence-Jones
protein in urine
** absence of paraproteins in plasma and in the urine.
14
15.
Epidemiology
• Incidence 4-7x 10-5
with the lowest incidence in Asians and
the highest in blacks.
• Essentially a disease of the elderly, median age at diagnosis is
between 63 and 70 years in Europe and north America,
compared to 50-60 years in sub-Sahara Africa.
• Slight male predominance in all populations, 1.7-2:1
15
16.
Clinical Features
• Spectrumfrom asymptomatic paraproteinaemia
detected on routine testing (~20%) to rapidly
progressive illness with extensive, destructive bony
disease.
• Bone disease (~75%): Most present with bone
(usually back) pain or pathological fracture; kyphosis
and loss of height may occur from vertebral
compression fractures.
• Weakness and fatigue (>50%)
• Recurrent infection (10%)
• Renal impairment (~10%)
16
Other Supportive Tests
•FBC and film
• ESR
• Serum electrolytes, urea & creatinine/uric acid
• Low serum albumin
• Hypercalcaemia (~20%)
• Serum immunoglobulins
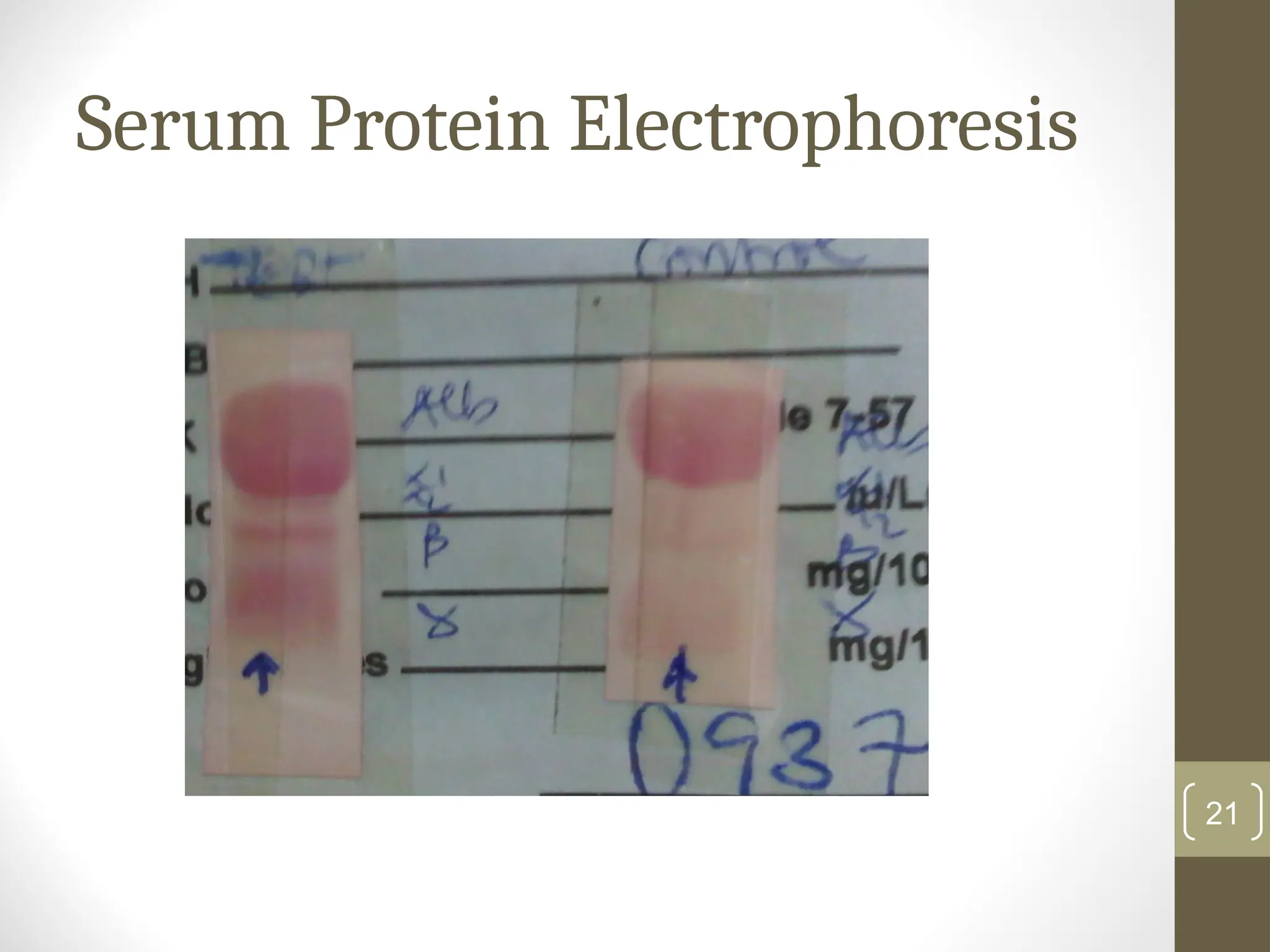
• Serum protein electrophoresis
• Routine urinalysis may detect proteinuria (~70%)
• Urinary Bence Jones proteinuria
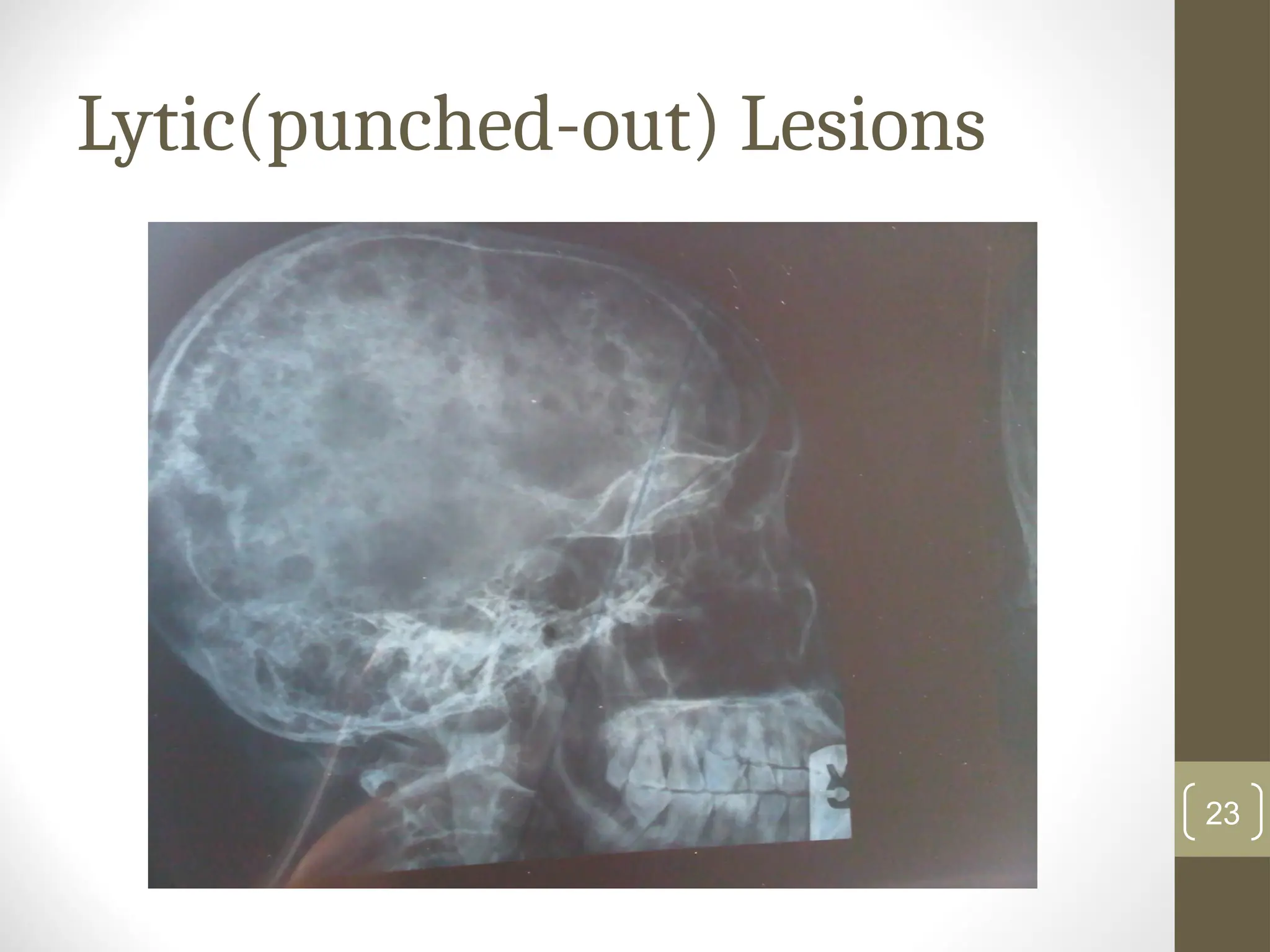
• X-ray sites of bone pain – pathological fracture(s) or lytic
lesion(s) 19
20.
Other Tests
• ImmunophenotypicCharacteristics:
• Strong expression of CD38, CD138, a single class of cytoplasmic
immunoglobulin (cIg). The
• Expression of CD40 and CD56 by a majority of myeloma cells
Myeloma
• Expression of CD20 by the minority of patients with the t(11;14)
translocation.
• Myeloma cells are negative for CD5, CD19, and surface Ig (sIg)
expression.
20
Usefulness of theBiological
tests
•These tests are useful for
differentiation of Symptomatic
myeloma, Smouldering (or
indolent) myeloma and MGUS,
and therefore treatment
approach 25
26.
Diagnostic Criteria forMGUS
Kyle RA, et al. International Myeloma Working Group. Br J Haematol 2003; 121: 749–757
• M-protein in serum <30 g/l
• Bone marrow clonal plasma cells <10%
and low level of plasma cell infiltration in a
trephine biopsy
• No evidence of other B-cell proliferative
disorders
• No related organ or tissue impairment or
bone damage including lytic bone lesions 26
27.
Diagnostic criteria forSmouldering Myeloma
Kyle RA, et al. International Myeloma Working Group. Br J Haematol 2003; 121: 749–757
• M-protein in serum ≥ 30 g/l
and/or
• Bone marrow clonal plasma cells ≥ 10%
• No related organ or tissue impairment- ROTI (no end organ
damage, including bone lesions)
• No evidence of any other chronic B-cell lymphoproliferative
disorder
27
28.
Diagnostic Criteria forSymptomatic Myeloma
Kyle RA, et al. International Myeloma Working Group. Br J Haematol 2003; 121: 749–757
• Presence of M-protein in serum and/or urine
• Presence of clonal marrow plasma cells or plasmacytoma
• Presence of ROTI (ie, myeloma Related end Organ or Tissue
Impairment lesions) manifested by CRAB.
28
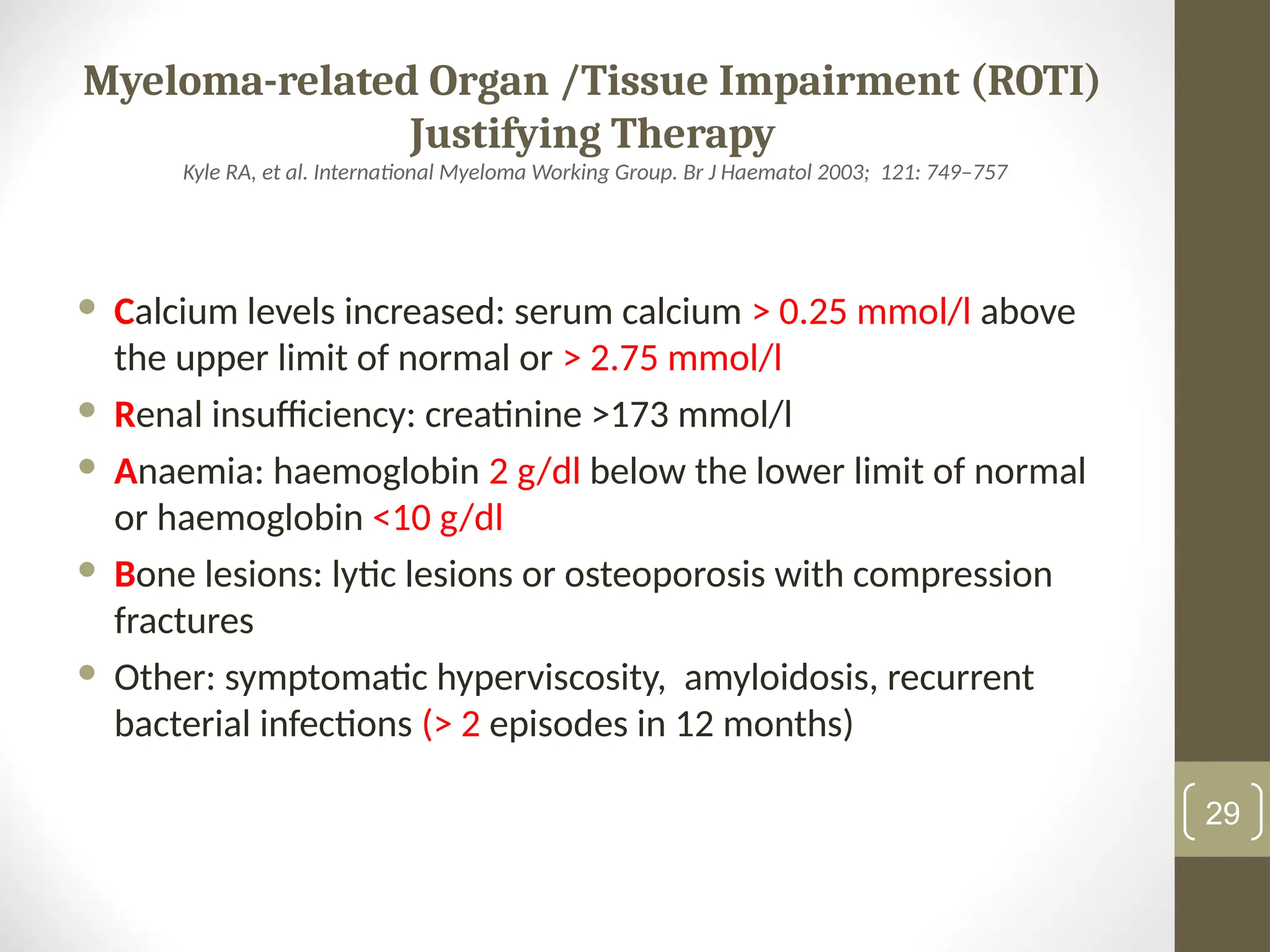
29.
Myeloma-related Organ /TissueImpairment (ROTI)
Justifying Therapy
Kyle RA, et al. International Myeloma Working Group. Br J Haematol 2003; 121: 749–757
Calcium levels increased: serum calcium > 0.25 mmol/l above
the upper limit of normal or > 2.75 mmol/l
Renal insufficiency: creatinine >173 mmol/l
Anaemia: haemoglobin 2 g/dl below the lower limit of normal
or haemoglobin <10 g/dl
Bone lesions: lytic lesions or osteoporosis with compression
fractures
Other: symptomatic hyperviscosity, amyloidosis, recurrent
bacterial infections (> 2 episodes in 12 months)
29
30.
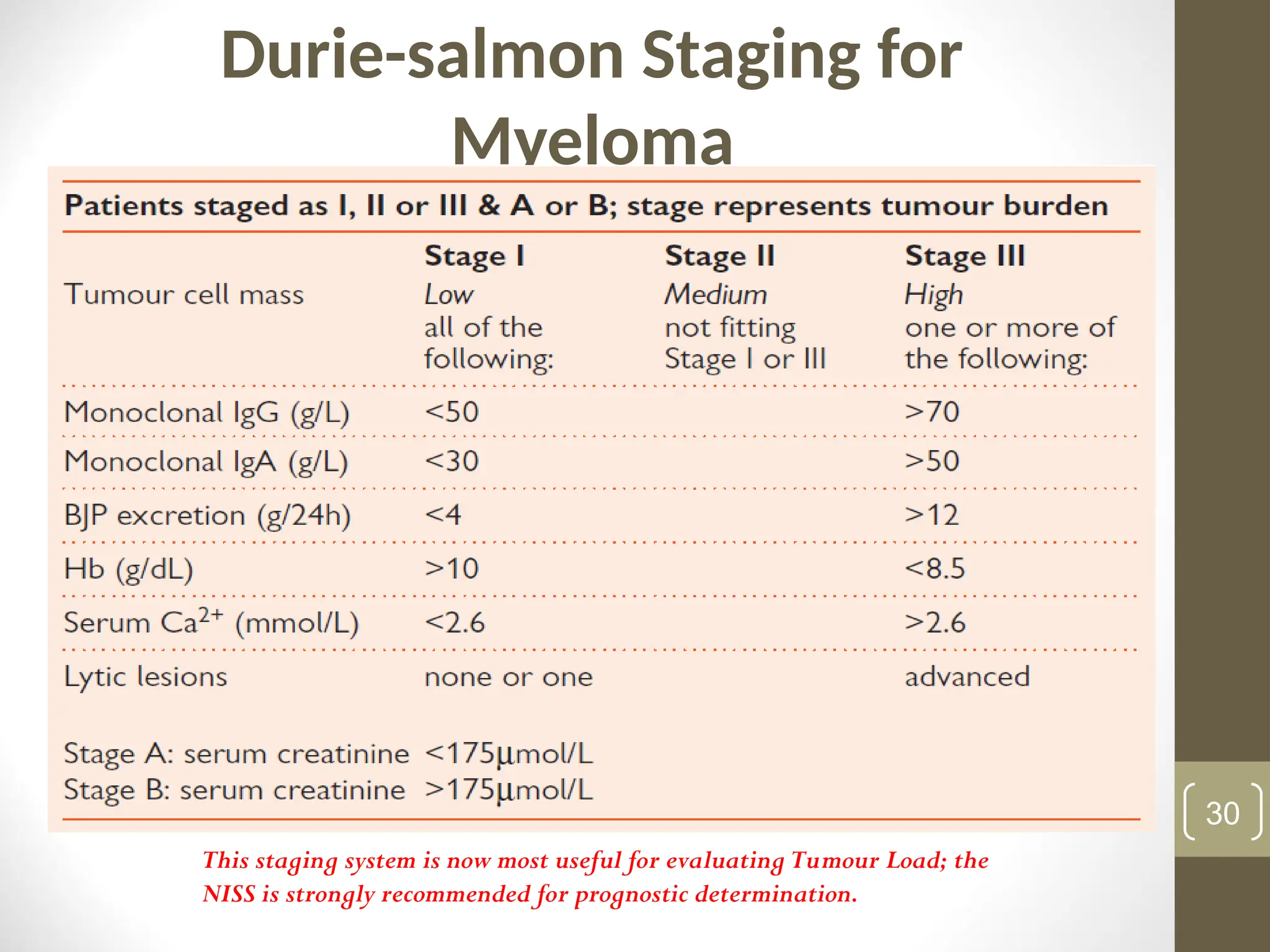
Durie-salmon Staging for
Myeloma
(Modifiedby Harousseau JL & Dreyling M. Ann Oncol 2010; 21 (Suppl 5): v155–v157)
30
This staging system is now most useful for evaluating Tumour Load; the
NISS is strongly recommended for prognostic determination.
31.
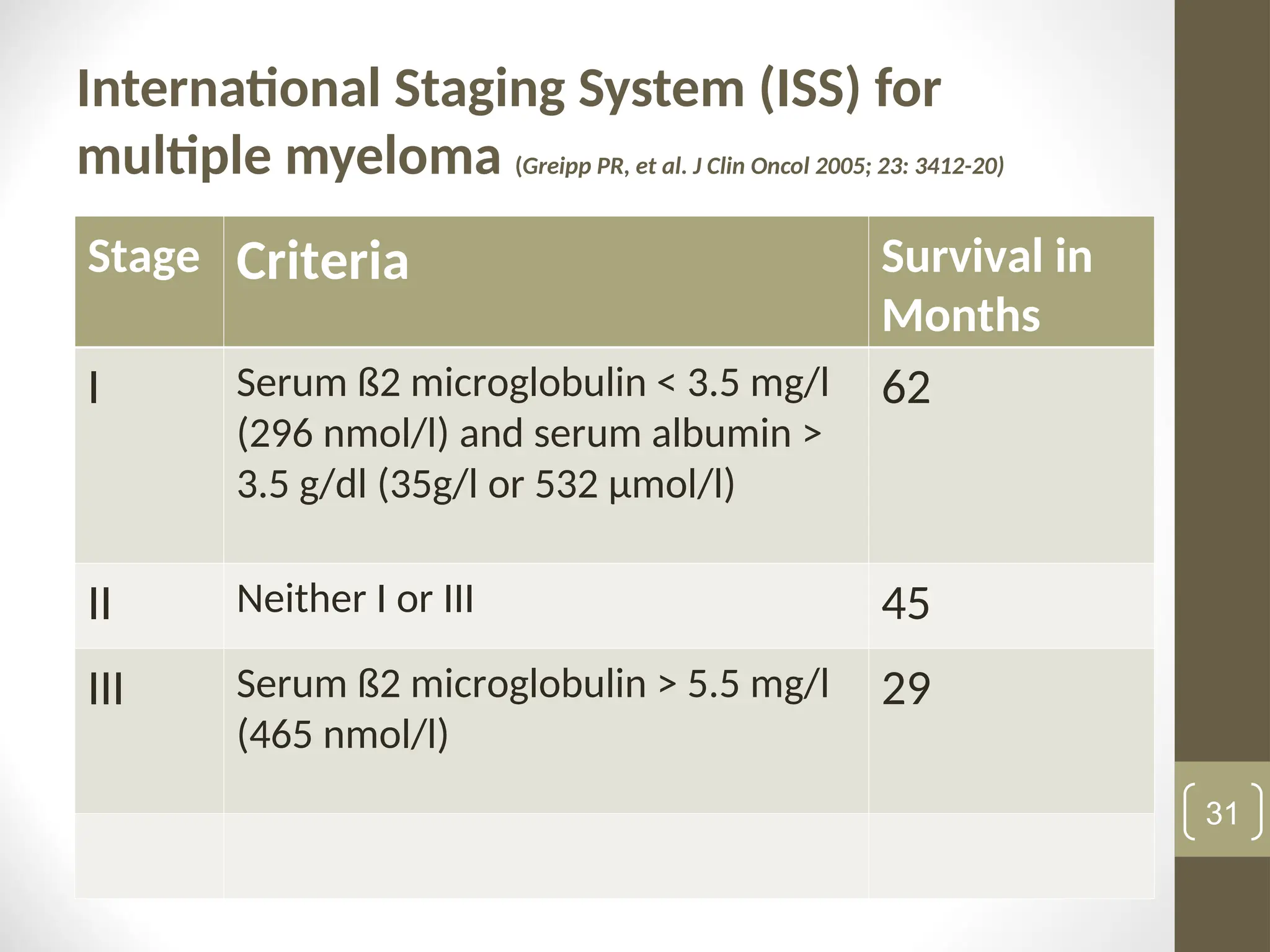
International Staging System(ISS) for
multiple myeloma (Greipp PR, et al. J Clin Oncol 2005; 23: 3412-20)
Stage Criteria Survival in
Months
I Serum ß2 microglobulin < 3.5 mg/l
(296 nmol/l) and serum albumin >
3.5 g/dl (35g/l or 532 μmol/l)
62
II Neither I or III 45
III Serum ß2 microglobulin > 5.5 mg/l
(465 nmol/l)
29
31
32.
Treatment of Multiple
Myeloma
Treatment is indicated Only in Patients with Symptomatic
Disease including Non-secretory myeloma. It involves
supportive and Definitive interventions
Supportive
Multidisciplinary approach: haematologists, orthopaedic, renal
physicians, microbiologists, physiotherapists, radiotherapists, etc.
Counselling
Anaemia & erythropoietin: rule out Nutrient deficiencies
Treatment of hypercalcaemia
Management of pain: opioids/non-opioids, but avoid NSAIDs for
its nephrotoxicity
32
33.
Treatment of Multiple
Myeloma
•Supportive
• Management of renal impairment (dialysis if indicated)
• Blood and blood products supply
• Treatment of infection (s)
• Bone disease – the use of radiotherapy, bisphosphonates
(pamidronate, zoledronate, etc)
• Hyperviscosity syndrome
33
34.
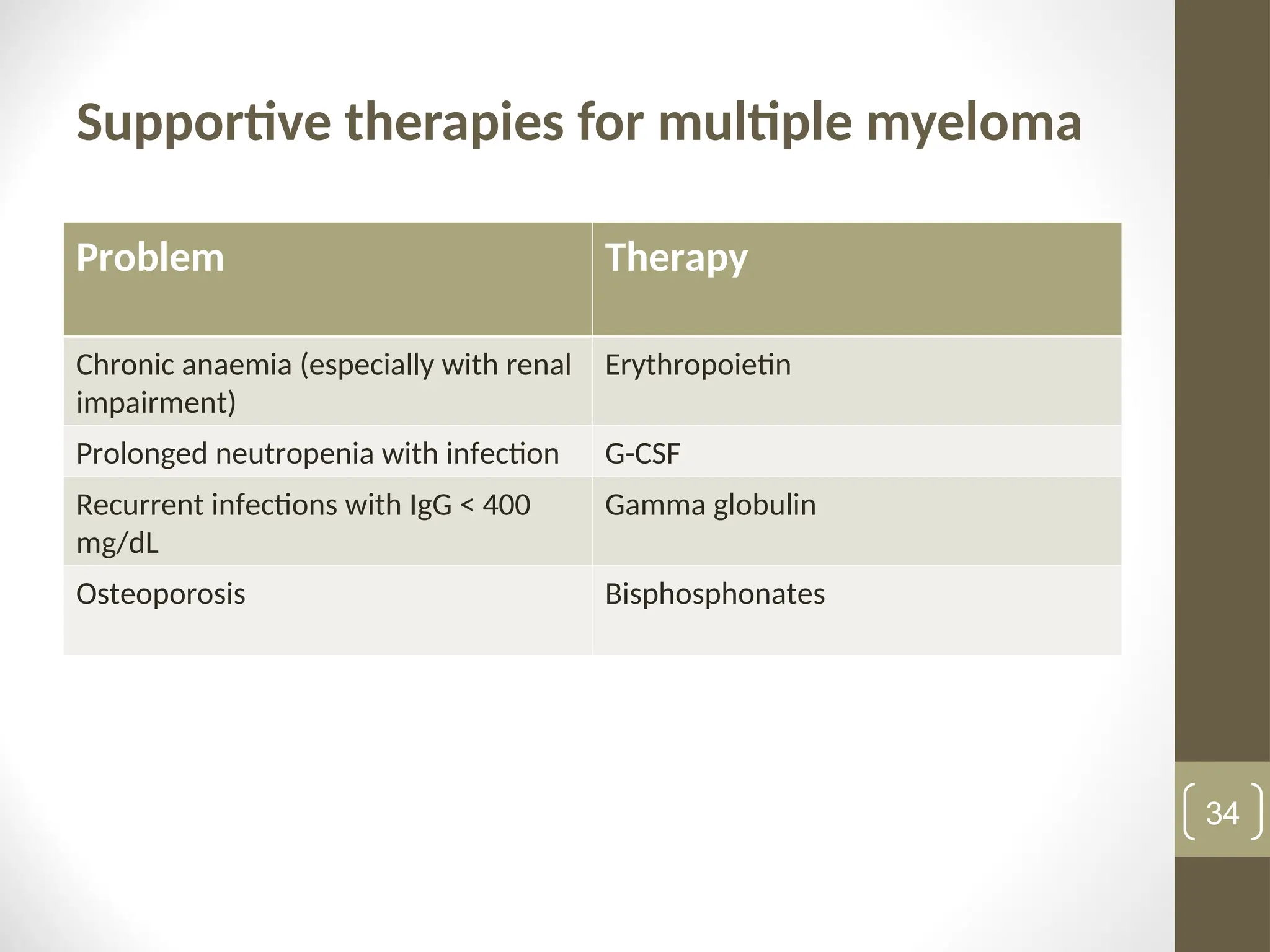
Supportive therapies formultiple myeloma
Problem Therapy
Chronic anaemia (especially with renal
impairment)
Erythropoietin
Prolonged neutropenia with infection G-CSF
Recurrent infections with IgG < 400
mg/dL
Gamma globulin
Osteoporosis Bisphosphonates
34
35.
Definitive Therapy: Factors
InfluencingChoice of Therapy
Age
Older individuals (> 65 yrs): unsuitable for SCT; high risk of
comorbidities and intolerance to high-dose chemotherapy
WHO Performance score: 0-2 Versus > 2
Disease Stage: I/II Versus Stage III disease
Comorbidities:
Renal Failure: good fluid, 3l/d and avoid NSAIDs
Diabetes mellitus
Pathological fractures
Cord compression (immediate dexamethasone 40mg dly x 4 days, while
processing other tests)
Infections
Economic status
35
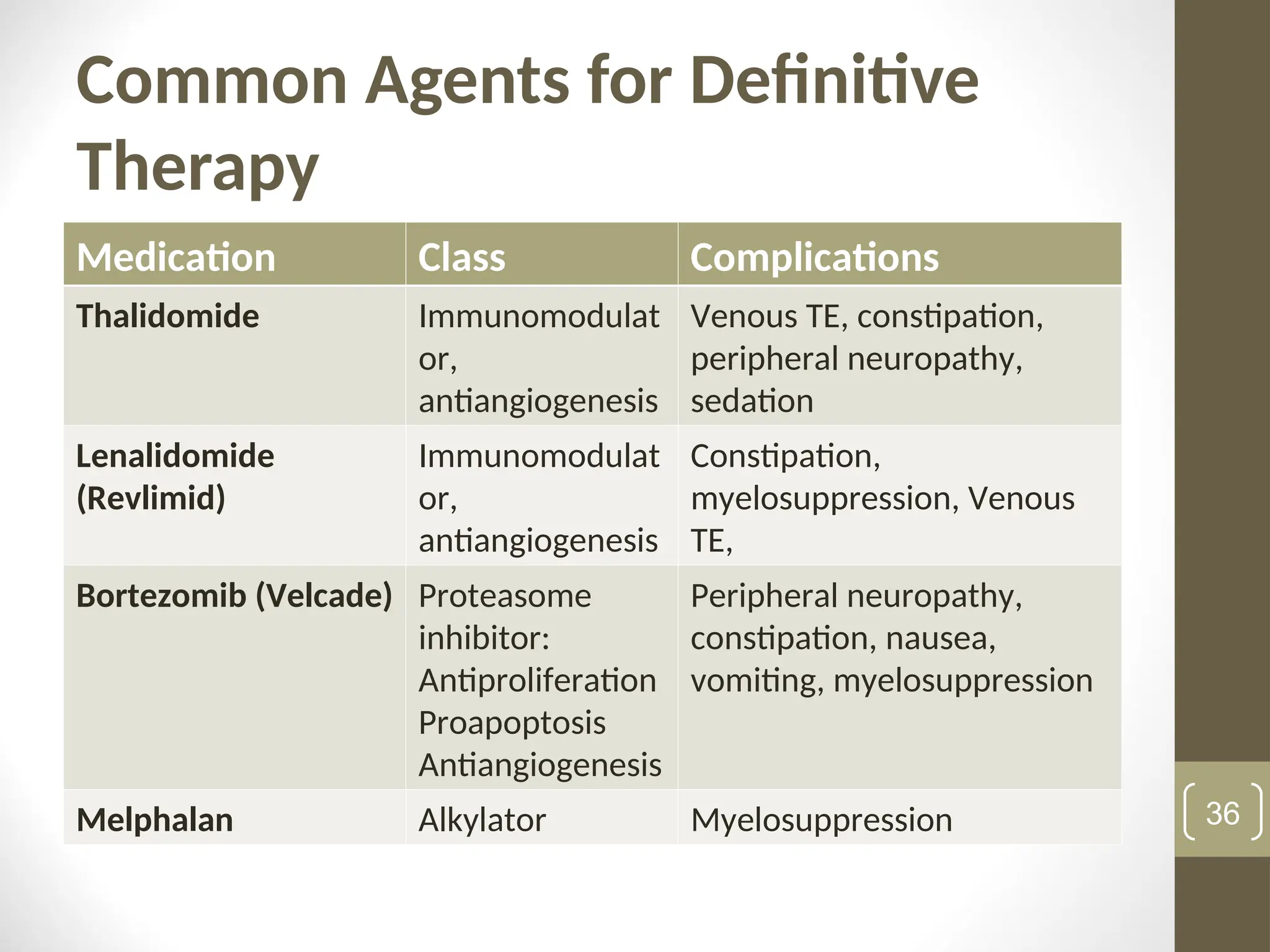
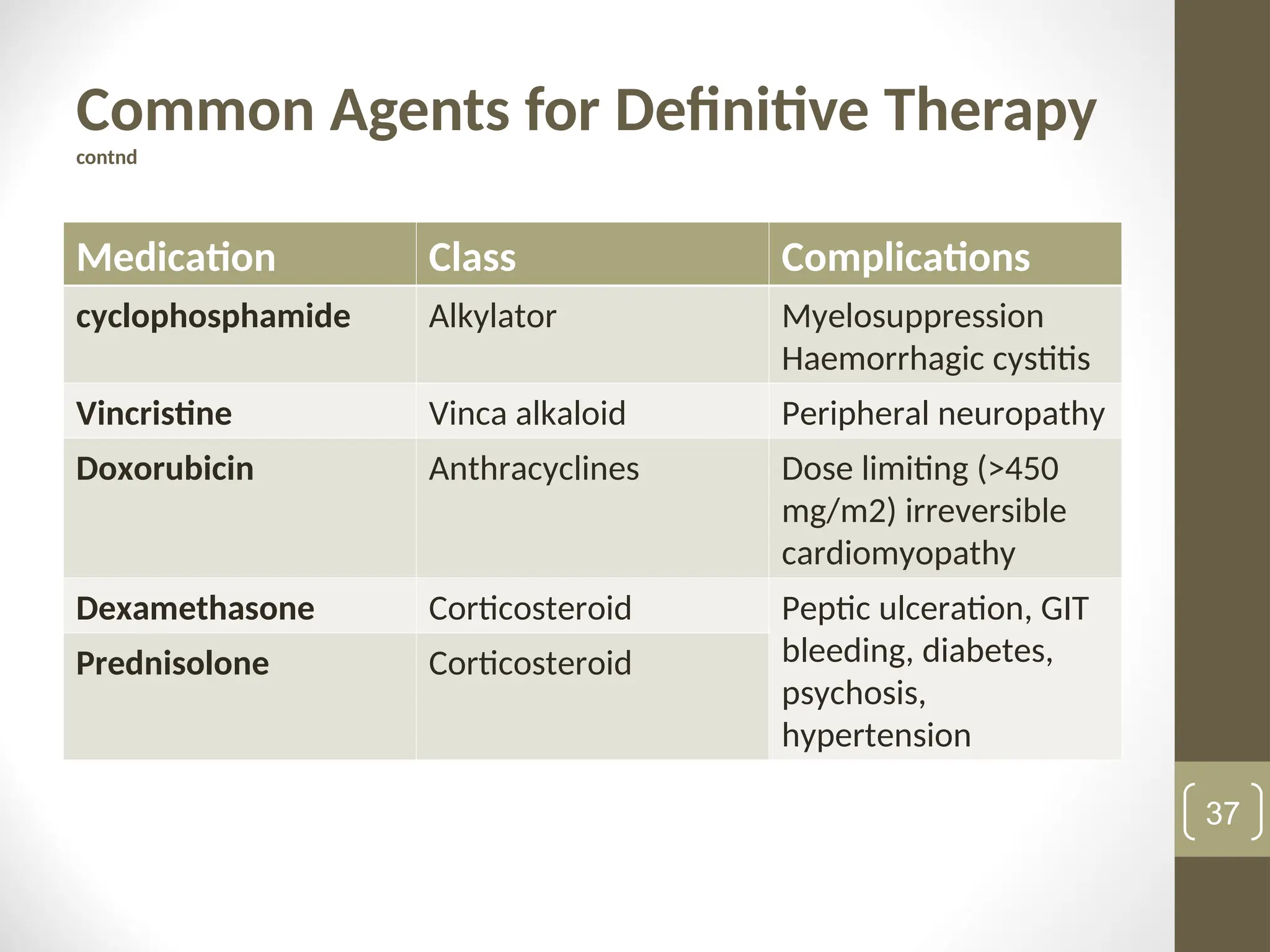
Common Agents forDefinitive
Therapy (contnd)
• Radiotherapy
• Stem Cell transplantation:
• Auto-SCT (may be repeated)
• Allo-SCT, mainly for the few very fit younger
patients < 50 years with suitable donors;
transplant related morbidity and mortality is
high.
38
39.
Conventional Definitive Therapy:Elderly
Patients Ineligible for HDT/ASCT
VAD: 28-day cycle
Vincristine 0.4 mg IV ds 1-4
Adriamycin 10mg/m2
IV ds 1-4
Dex 40mg PO ds 1-4
(vincristine & adriamycin together in 100 ml N/saline, infused rapidly)
MP: 28-d cycle
Melphalan 8 mg/m2
PO ds 1-4
Prednisolone 60mg/m2
PO ds 1-4
CP: 28-day cycle
Cyclophosphamide 200mg/m2
PO ds 1-4
Prednisolone 60mg/m2
PO ds 1-4
39
40.
Definitive Therapy Basedon Novel Drugs
MP-T (28-day cycle) (not for individuals desirous of ASCT)
Melphalan 4mg/m2
PO ds 1-7
Prednisolone 40mg/m2
PO ds 1-7
Thalidomide 100mg PO d 1-28
TD (28-day cycle):
Thalidomide 100-200mg PO ds 1-28
Dexamethasone 40mg PO ds 1-4
PAD (28-day cycle):
*Bortezomib 1.3mg/m2
IV ds 1, 4, 8, 11
Adriamycin 9mg/ m2
(CIV)
&
Dexamethasone 40mg PO ds 1-4 every
cycle and
ds 8-11, 15-
18 for cycle 1
only
Bortezomib (Velcade, previously PS-341):
40
Relapsed/Refractory
• Note durationof initial remission, if long, re-try the initial
induction regimen; if short change to new regimen, eg if
immunomodulator was the 1st approach, try protease inhibitor
• Local radiotherapy: individuals with local relapse such as spinal
plasmacytoma, with little evidence of active disease elsewhere
43
44.
Response Evaluation
Harousseau JL& Dreyling M. Ann Oncol 2010; 21 (Suppl 5): v155–v157)
• Based on serum and urine electrophoresis.
• Complete remission (CR): Negative immunofixation on the serum
and urine; < 5% marrow plasma cells, no soft tissue
plasmacytoma
• Very good partial remission: ≥90% reduction of the serum M-
protein; detectable serum and urine M-protein on
immunofixation but by electrophoresis; < 100mg per 24 hours;
absent soft-tissue plasmacytoma
• Partial response: ≥ 50% reduction of the serum M-protein;
reduction in 24-h urine M-protein by ≥90% reduction of the
serum M-protein; ≥50% reduction in soft tissue plasmacytoma
44