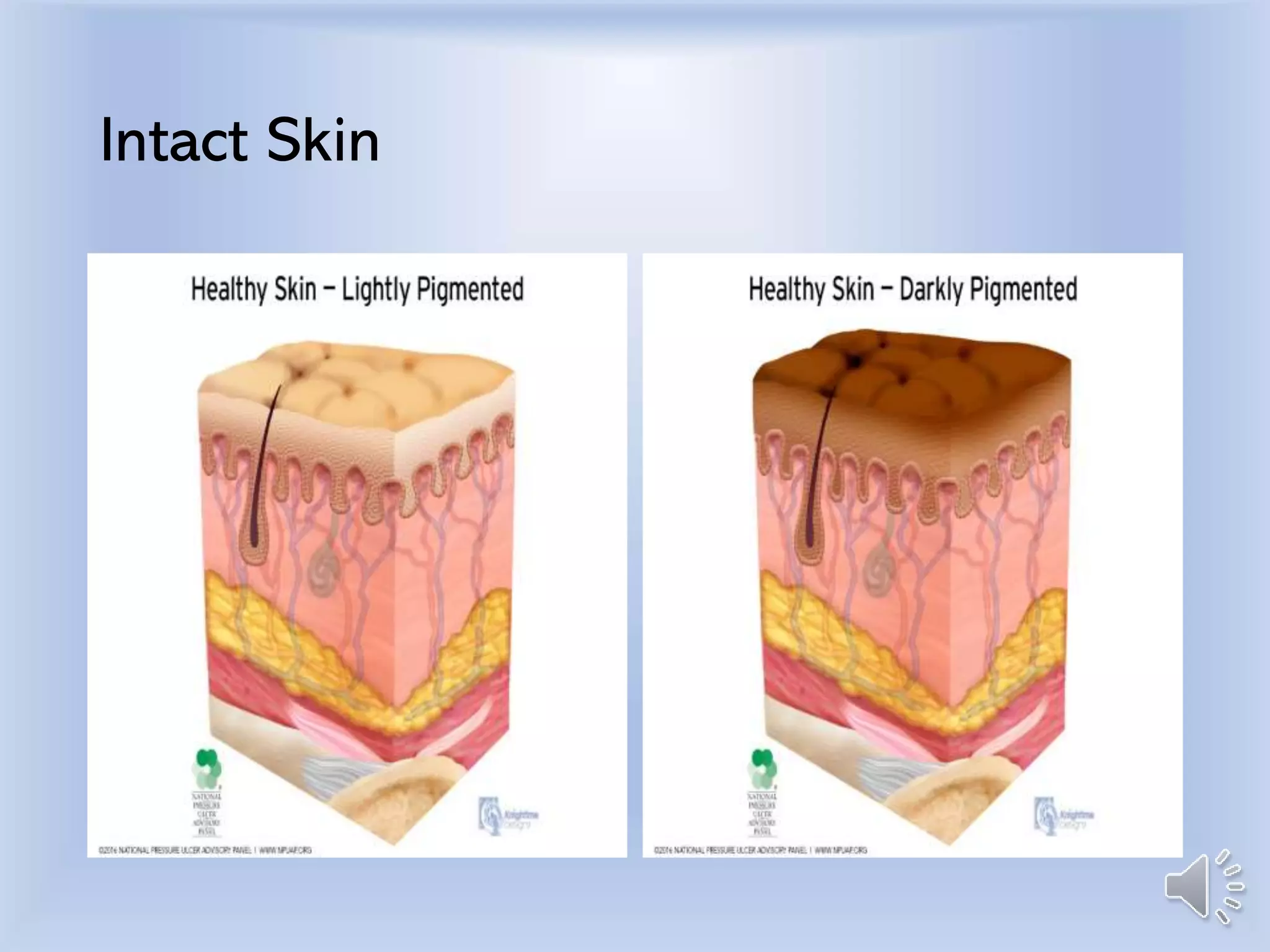
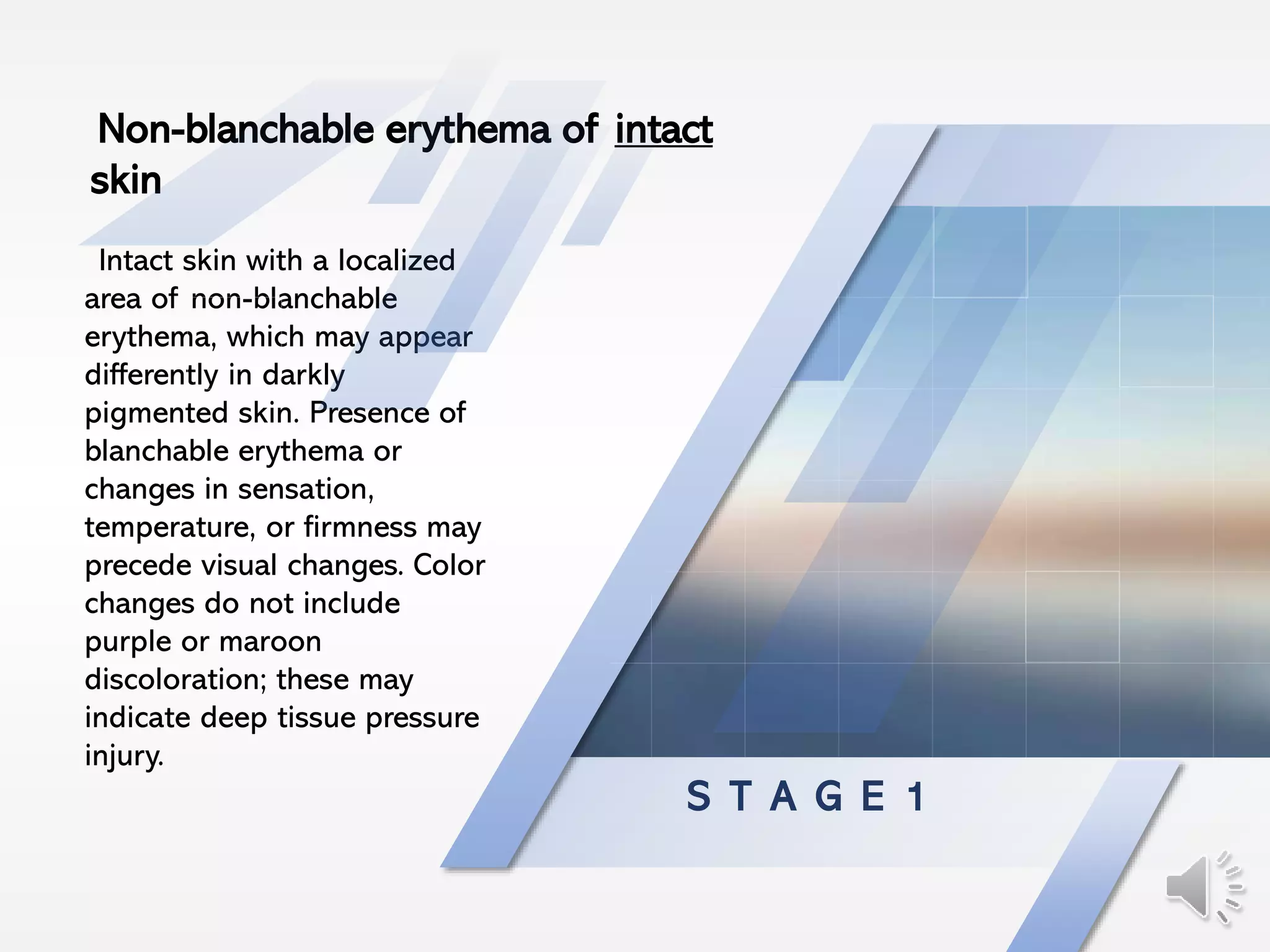
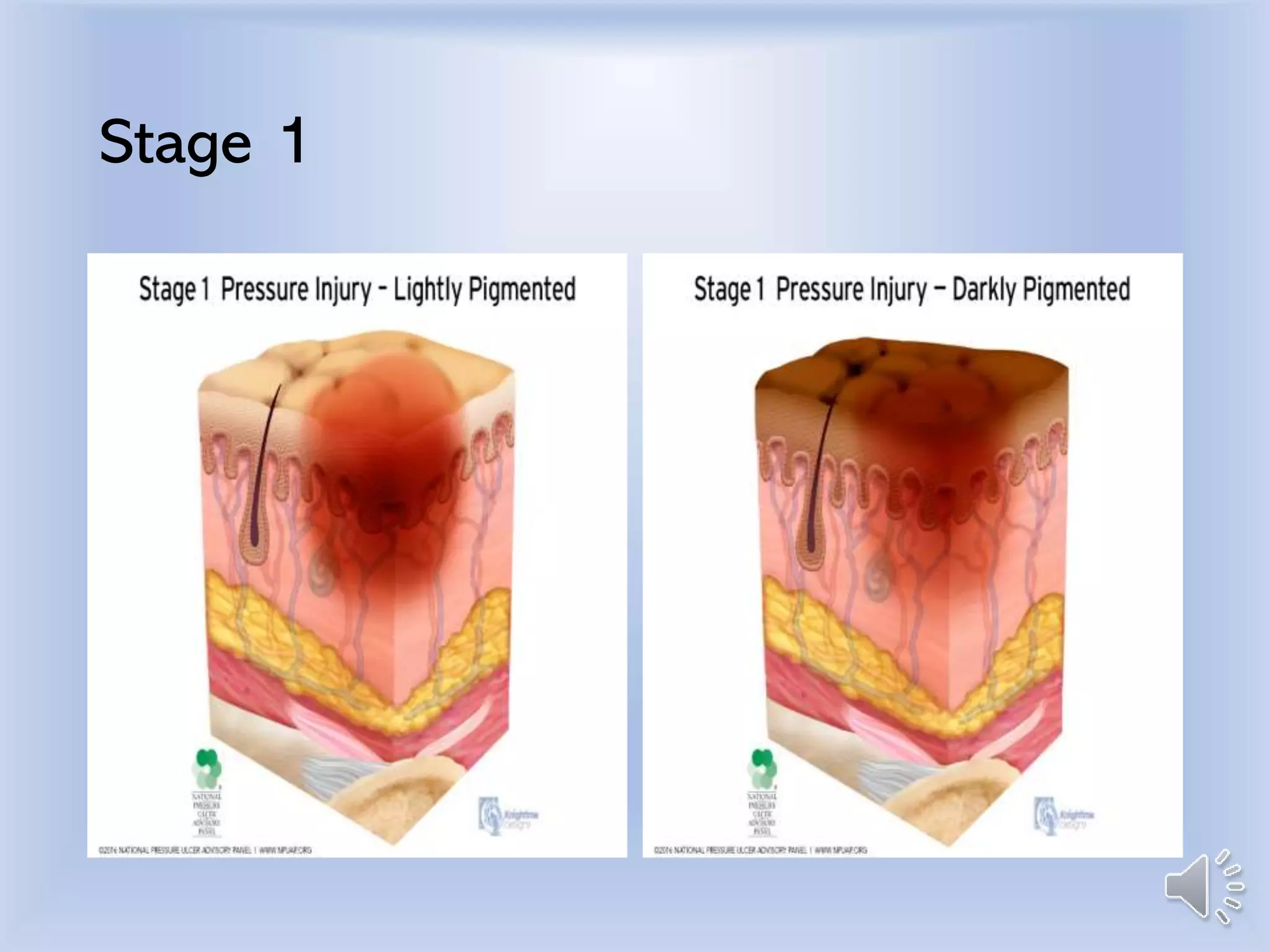
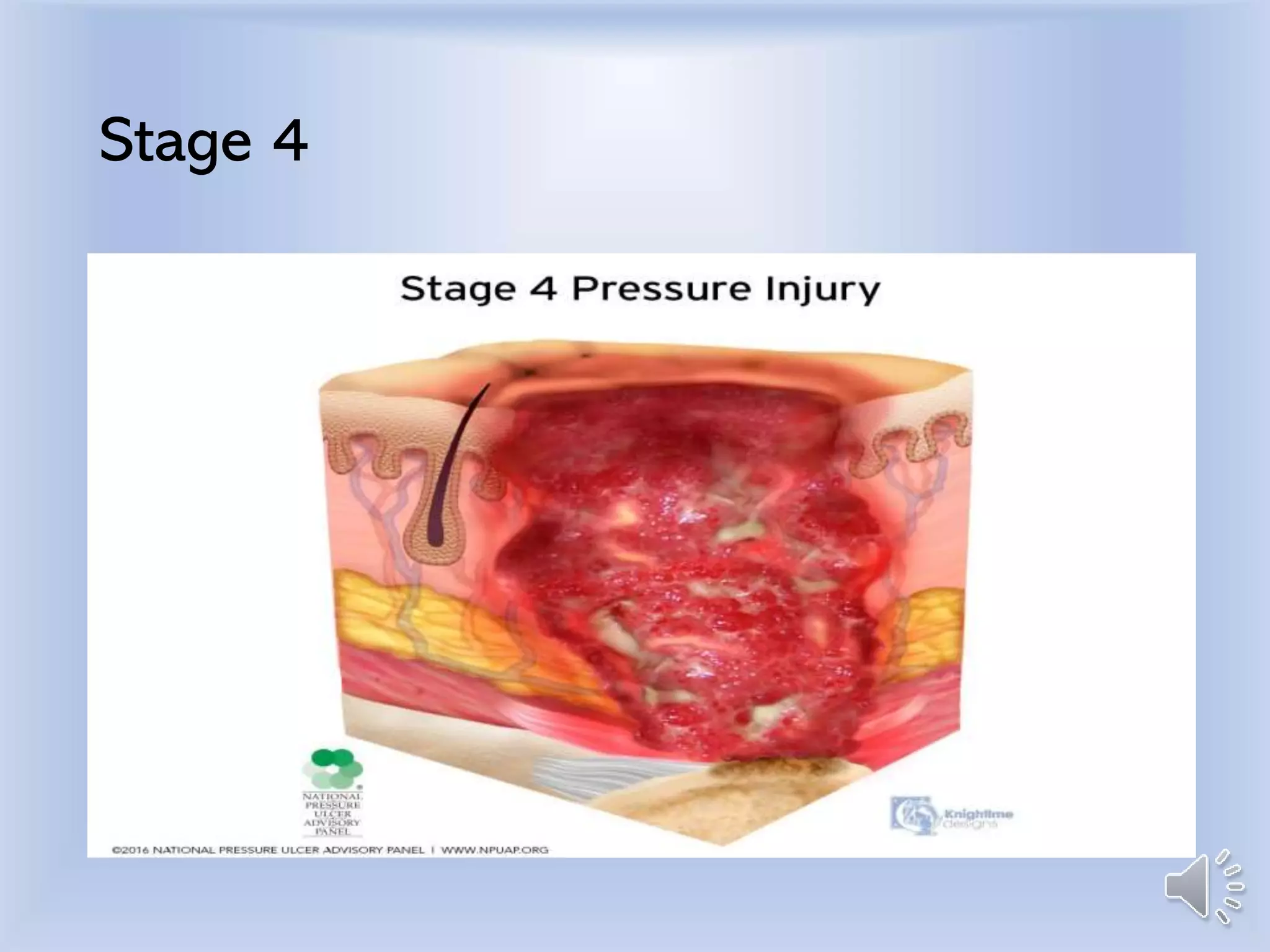
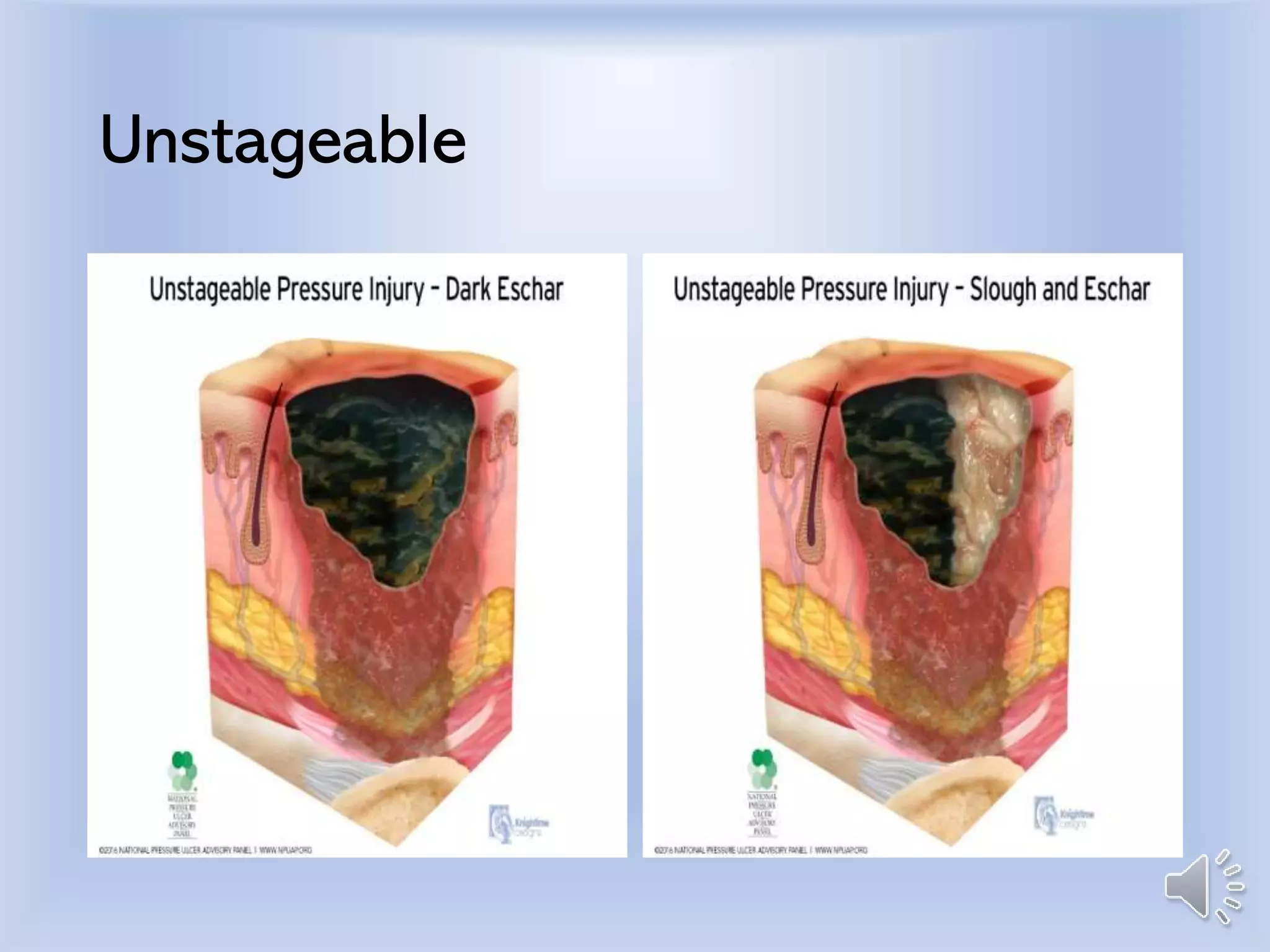
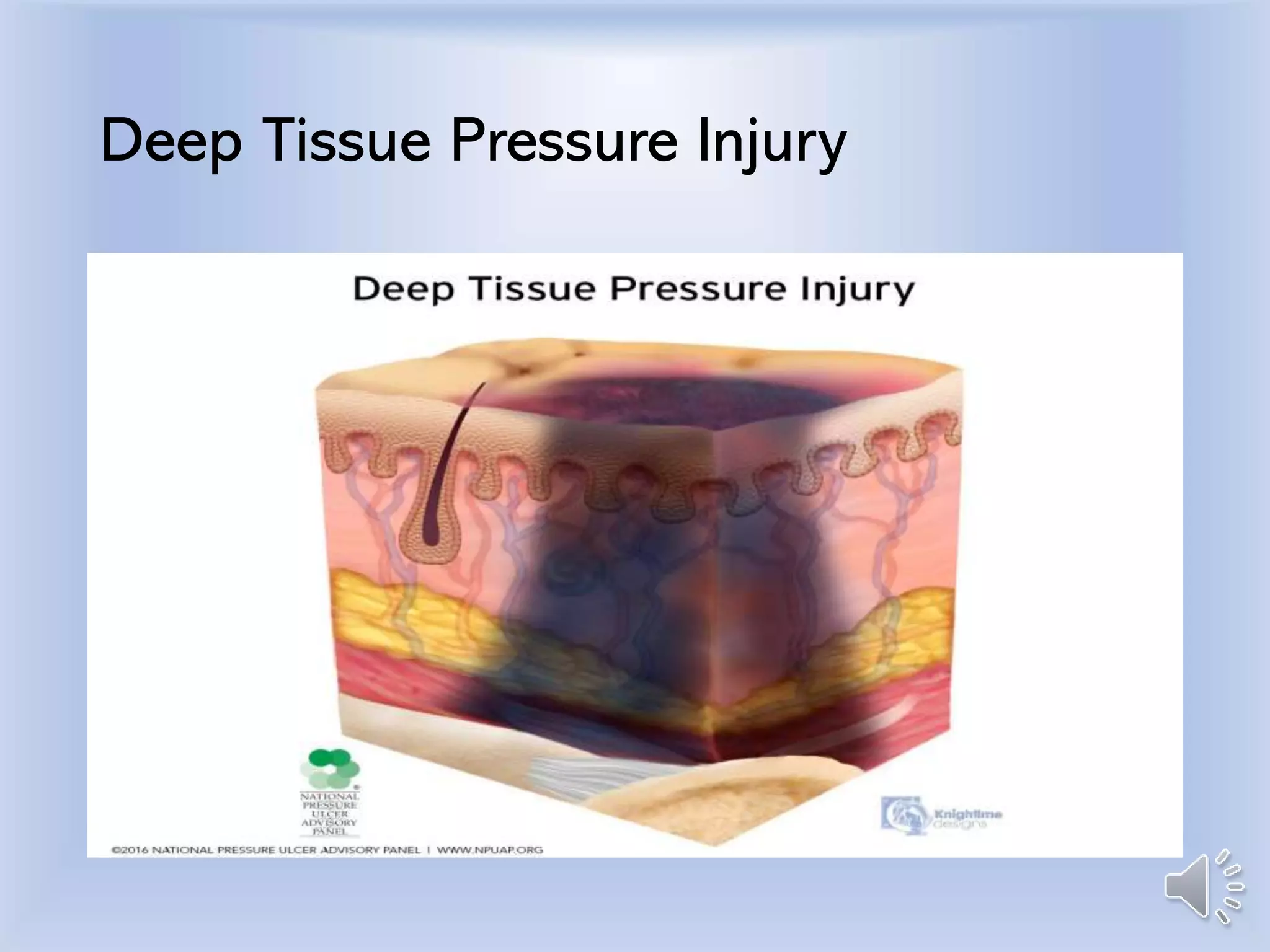
This document defines and describes the stages of pressure injuries, from Stage 1 (intact skin with non-blanchable erythema) to Stage 4 (full thickness skin and tissue loss with exposed bone, tendon or muscle). It also covers unstageable injuries, deep tissue pressure injuries, and injuries related to medical devices. The stages are defined by the extent of skin and tissue damage, from non-blanchable redness to complete tissue loss. Accurate staging is important for treatment and prevention of further injury.


![Skin integrity and wound care [autosaved] (2)](https://cdn.slidesharecdn.com/ss_thumbnails/skinintegrityandwoundcareautosaved2-130319145819-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Skin integrity and wound care [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/skinintegrityandwoundcareautosaved-130319145813-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)