The document provides a summary of a mock orthopaedics case presentation. It includes demographic details of a 45 year old male patient complaining of lower back pain radiating to his right ankle. On examination, the patient has reduced range of motion, muscle weakness on the right side, and a left lateral shift in his spine. Differential diagnoses include prolapsed disc, piriformis syndrome, and sciatic nerve impingement. Treatment will focus on reducing pain, increasing mobility, and correcting posture through techniques like heat, ultrasound, stretching, and interferential therapy.

![• Duration of pain- Acute [Since 1 week]
• Onset of pain – Sudden
• Nature of pain- Constant
• Type of pain sensation – Pins and needle
sensation.
• Radiation of pain – Peripherlization.](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-5-320.jpg)
![• Intensity of pain- Measured through VAS [visual
analogue scale]
INTERPRETATION
From 0 to 10 cm Patient marked pain level at 7.2cm.](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-6-320.jpg)
![• Past medical history – Nothing relevant.
• Surgical history – None
• Associated Probems- Patient has diabetes for
which he takes medication[AMLODIPIN]
• Personal history – Patient does not smoke or
drink.
• Patient goes for a walk daily.
• Family history – Not relevant
• Occupation history – IT job [ 7-8 hrs continuous
sitting][Due to Pain patient is not able to sit for
more than 20-25 min continous]](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-9-320.jpg)
![Observation
• Body type – Mesomorph
• Body mass index[BMI] – weight/[height sq.]
Weight - 75 kg
Height - 1.60 m[160cm]
BMI - 29 kg per m sq.](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-11-320.jpg)
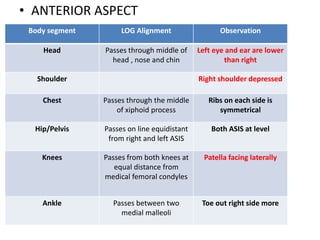
![• Posture – FRONTAL VIEW
Right shoulder slightly depressed as compared
to left
Left side List[Lateral shift of spine]
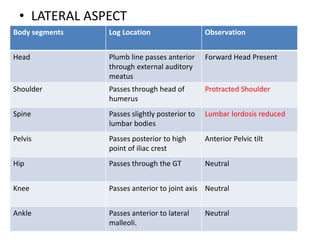
SAGITTAL VIEW
Protracted Shoulders with Forward Head](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-12-320.jpg)
![ON PALPATIONS
• Tenderness – Present
Site of tenderness- over area of L3, L4,L5 , S1
at Greater trochanter
Grade of tenderness- Grade 2 [Tenderness
with wince on deep palpation]
• Warmth – Normal body warmth on pain site
• Odema – No odema present.
• Spasm – Present at paraspinal muscles](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-16-320.jpg)
![Motor assessment
Range of motion [ROM]
Interpretation
All the ROM are less than normal range.
JOINT/MOTION ROM Normal ROM END FEEL
Thoracolumbar
Flexion
46.5 – 53= 6.5 cm 10 cm Firm
Thoracolumbar
Extension
46.5 – 43.5 = 3
cm
Firm
Lumbar flexion
[modified schober
test]
15 – 19 = 4 cm 5-7 cm Firm
Lumbar extension
[modified
schober test]
15 – 14 = 1 cm 1.6 cm Firm](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-18-320.jpg)
![Normal
ROM
END FEEL
[LEFT]
AROM
[LEFT]
JOINT/
MOTION
AROM
[RIGHT]
END FEEL
[RIGHT]
0-30 Firm 0 - 26 Thoraco-
lumbar
Lateral
Flexion
0 - 24 Firm
0-35 Firm 0 - 30 Thoraco-
lumbar
Rotation
0 - 25 Firm](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-19-320.jpg)
![Normal
range
END
FEEL
PROM
[LEFT]
AROM
[LEFT]
HIP
JOINT
MOTION
AROM
[RIGHT]
PROM
[RIGHT]
END FEEL
0-120 firm 0 - 120 0 - 115 Flexion 0 -105 0 - 115 soft
0-20 firm 0 - 20 0 - 16 Extension 0 - 15 0 - 18 firm
0-45 firm 0 - 45 0 - 40 Abduction 0 - 35 0 - 40 firm
45-0 firm 45- 0 40 - 0 Adduction 35 - 0 40 - 0 firm
0-40 firm 0 - 40 0 - 35 Internal
rotation
0 – 25 0 -30 firm
0-50 firm 0 -50 0 - 45 External
rotation
0-40 0 - 45 firm](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-20-320.jpg)
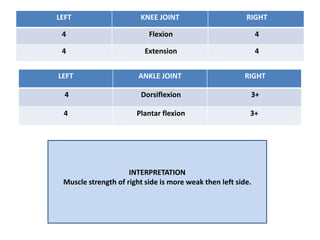
![Normal
ROM
END
FEEL
PROM
[LEFT]
AROM
[LEFT]
KNEE
JOINT
MOTION
AROM
[RIGHT]
PROM
[RIGHT]
END
FEEL
0-150 soft 0 - 150 0 - 140 Flexion 0 - 140 0 - 150 soft
150-0 firm 150- 0 140- 0 Extension 140- 0 150 - 0 firm
Normal
ROM
END
FEEL
PROM
[LEFT]
AROM
[LEFT]
ANKLE
JOINT
MOTION
AROM
[RIGHT]
PROM
[RIGHT]
END
FEEL
0-20 firm 0 - 20 0 - 15
Dorsiflexion
0 - 18 0 - 20 firm
0-50 firm 0 - 50 0 - 40 Plantar
flexion
0 - 45 0 - 50 firm](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-21-320.jpg)
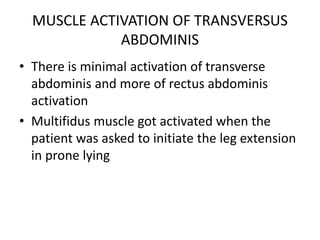
![LEFT HIP JOINT RIGHT
4 Flexion [4]
4 Extension 4
4 Abduction [3+]
4 Adduction [3+]
4 Internal Rotation [3+]
4 External Rotation [3+]](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-24-320.jpg)
![• POSTERIOR ASPECT
Body Segment LOG Location Observation
Head Plumb line passes through
middle of head
Right Neck shoulder
distance[7] is more than
left[6]
Shoulder Right shoulder depressed
Scapula Right scapula medially
rotated
Spine Bisecting vertebral
Column into equal halves
Left lateral shift /LIST
Hip/Pelvis Passes through the gluteal
cleft and equal distance
from PSIS
PSIS at level and gluteal
folds at level and
symmetrical
Knee Passes equidistant from
medial joint aspect
Neutral
Ankle Passes equidistant from
both the malleoli
Toe out right side more](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-31-320.jpg)
![GAIT EXAMINATION
[QUANTITATIVE ANALYSIS]
DISTANCE AND TIME
VARIABLE
RIGHT LEFT
STRIDE LENGHT 97.5 cm 97.8cm
STEP LENGTH 51.2cm 47cm](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-33-320.jpg)

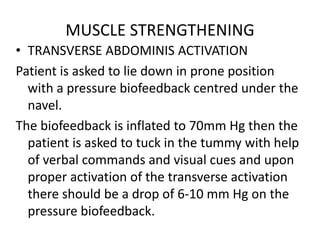
![NEUROLOGICAL EXAMINATION
• Myotomal examination Examination
Myotomes Observation
L1 Hip Flexion Intact
L2 Hip Flexion Adduction
Medial Rotation
intact
L3 Leg Knee Extension intact
L4 Dorsiflexion intact
L5 Great/Big toe extension Weakness
S1 Ankle Planter flexion Eversion
Knee Flexion
Weakness[ Performed
one leg standing and on
toes but not able to
maintain ]
S2 Ankle Planter flexion
Knee Flexion
intact](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-37-320.jpg)
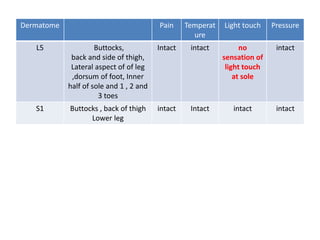
![• Dermatome Examination
.
Dermatom
es
[left]
Region Pain Temperatur
e
Light touch Pressur
e
L1 Back, over
trochanter
intact intact intact intact
L2 Front of thigh
to knee
intact Intact intact Intact
L3 Upper buttocks,
front of thigh
and knee,
medial lower
leg
intact Intact Intact Intact
L4 Inner buttocks
,outer thigh,
inside of leg ,
dorsum of foot
, big toe
intact intact Intact Intact](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-38-320.jpg)
![FUNCTIONAL ASSESSMENT
• The OSWESTRY
DISABILITY INDEX[ODI]](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-41-320.jpg)
![• Disability total score : 47
• Score obtained : 22
• Disability 22/47= 0.468
• Disability percentage= 46.8%
Interpretation of score
0%-20%=Minimal disability[can cope with ADLs]
21%-40%=Moderate disability[ Patient experience more pain and
difficulty in sitting , standing and lifting.]
41%-60%=Severe Disability [Pain remains the main problem in
this group but activities of daily living are affectted]
81%-100% =Patient are bedridden or exaggerating their
symptoms.](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-42-320.jpg)
![SPECIAL TEST
• Straight leg raising test- Positive [to check for
sciatic nerve ]
Hip flexion [55 degree as patient complains of
pain in back ]and adduction
Knee extension
Ankle dorsiflexion
Pain complains of shooting pain in gluteal
region.](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-44-320.jpg)
![For SI joint
• Flamingo test : Negative
Stand on one leg , stress more on stance side
Patient complains no pain in pubis area or SI joint
• Gaenslen’s test : Negative
Patient in side lying [test leg uppermost]
Knee to chest in lower leg by patient
Stabilize the pelvis while extending the hip of test leg.
No Pain in SI Joint and L4 nerve root
• Yeoman’s : Negative
Patient in prone with knees 90 degree flexed
Examiner extend the hip.
No pain in lumbar region , Si joint and anterior thigh.](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-47-320.jpg)
![• Correction Of LIST/Lateral shift.
BY therapist
Standing with flexed elbow in the side of lateral
shift [left elbow flexed]
Then therapist should wrap the arm around the
patient’s pelvis on the opposite side[right
side]and simultaneously pull the pelvis
towards while pushing the thorax away.
Once the shift is corrected ,immediately make
the patient bend backward.](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-60-320.jpg)
![• Self correction
Side lying on the side to which the thorax is
shifted[left side].
Place a small pillow or towel roll under the
thorax.
Patient remain in this position until pain
centralize
Then roll prone and perform passive extension
or prone press ups.](https://image.slidesharecdn.com/mockorthopaedicscasepresentationlowerbackpain-231004181704-476217fe/85/MOCK-ORTHOPAEDICS-CASE-PRESENTATION-LOWER-BACK-PAIN-pptx-61-320.jpg)































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









