Downloaded 16 times












![Work groups for Helsinki
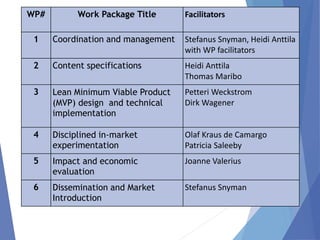
Content specification (WP 2) [Heidi & Thomas]
Questions, answers & Proms
IT Team (WP3) [Petteri & Dirk]
Get everything ready for the word “go”
Research and Literature (WP 4 & 5) [Olaf & Joanne]
Overall research framework
“Generic” funding proposal
Finish outstanding articles
Prepare Manchester abstracts (due date 15 June)
“Contract research” from other WPs](https://image.slidesharecdn.com/micfhelsinki-wednesday-welcomeandintroductions-150603130601-lva1-app6891/85/mICF-Workshop-3-June-2015-Overview-PowerPoint-43-320.jpg)


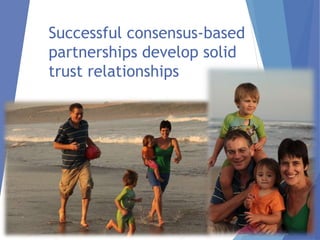
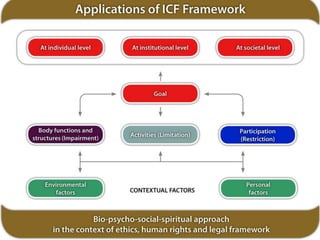
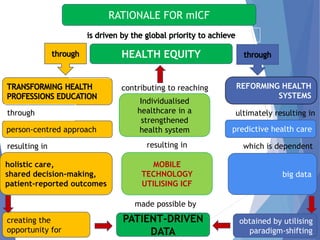
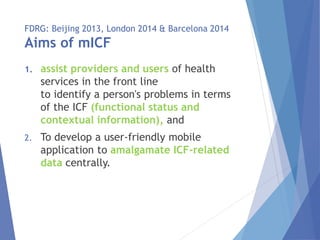
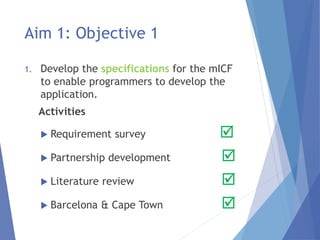
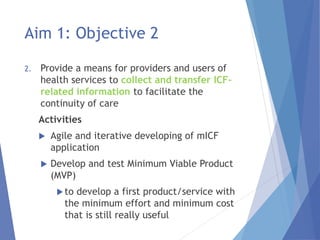
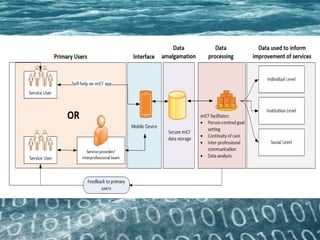
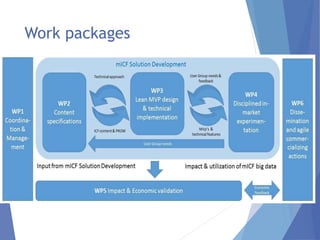
This document provides an overview of a workshop for the mICF Collaborative taking place in Helsinki, Finland from 2-4 June 2015. The workshop aims to bring together partners working on developing a mobile application to collect patient data based on the International Classification of Functioning framework. The summary discusses the motivation and goals of the mICF project, which include facilitating integrated care through collecting patient-reported data using mobile technology. It outlines the work packages and objectives for developing content specifications, a minimum viable product, testing the application, and evaluating impact. The workshop aims to advance work on content development, technical implementation, research planning and dissemination activities.





















































































