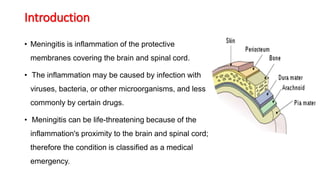
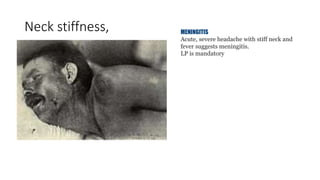
Meningitis is an inflammation of the protective membranes covering the brain and spinal cord. It is usually caused by a viral or bacterial infection and can be life-threatening if not treated promptly. The symptoms of meningitis vary depending on the age of the patient but may include severe headache, fever, neck stiffness, nausea, confusion, and petechial rash. A lumbar puncture is required to diagnose meningitis by examining the cerebrospinal fluid for elevated white blood cells, low glucose levels, and high protein levels. Early diagnosis and treatment of the cause is important to prevent serious complications.