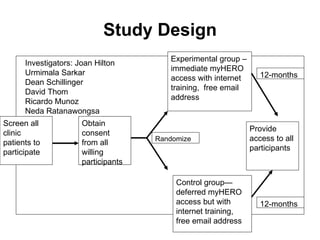
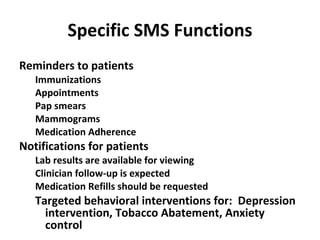
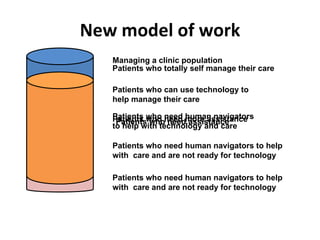
The document discusses using technology like computers, phones, and televisions to improve health. It reviews current research projects using personal health records (PHRs) and text messaging to empower patients and enhance care. The research aims to reduce health disparities through improved access to technology and information. Key goals are promoting self-management, providing a platform for implementation research, and empowering patients.



![Thank you and Questions Jim Kahn 415-699-1118 [email_address] http://profiles.ucsf.edu/ProfileDetails.aspx?Person=4999786](https://image.slidesharecdn.com/medicalgrandrounds9-22-2011-110921225448-phpapp02/85/Medical-grand-rounds-9-22-2011-56-320.jpg)