












![[Health Data is] the
most valuable
information in the
digital age, bar none. Deborah
Peel, Patient Privacy Rights
84](https://image.slidesharecdn.com/mhealthtutorial-141012231842-conversion-gate02/75/mHealth-Beyond-Consumer-Apps-Tutorial-MobileHCI-84-2048.jpg)



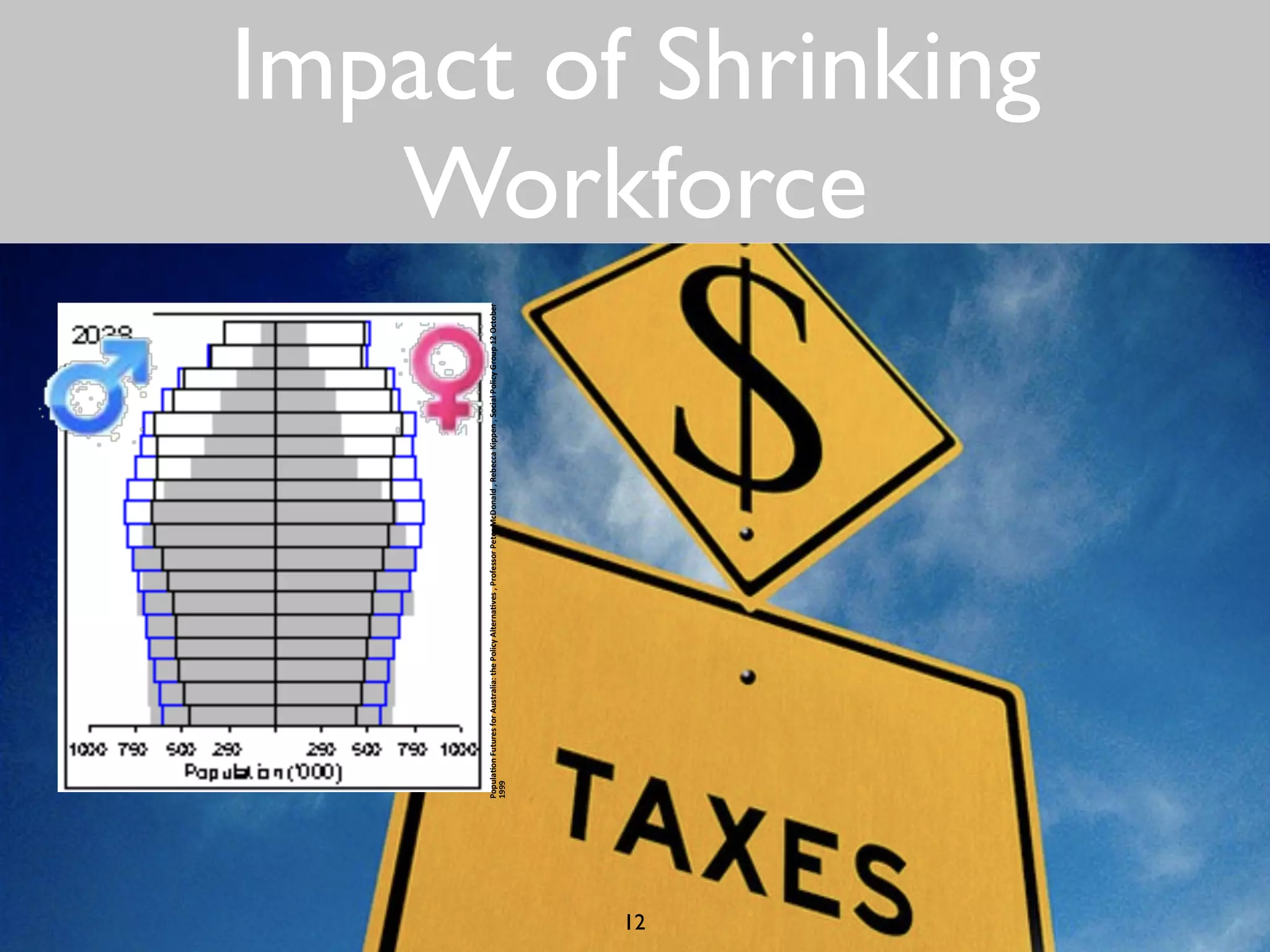
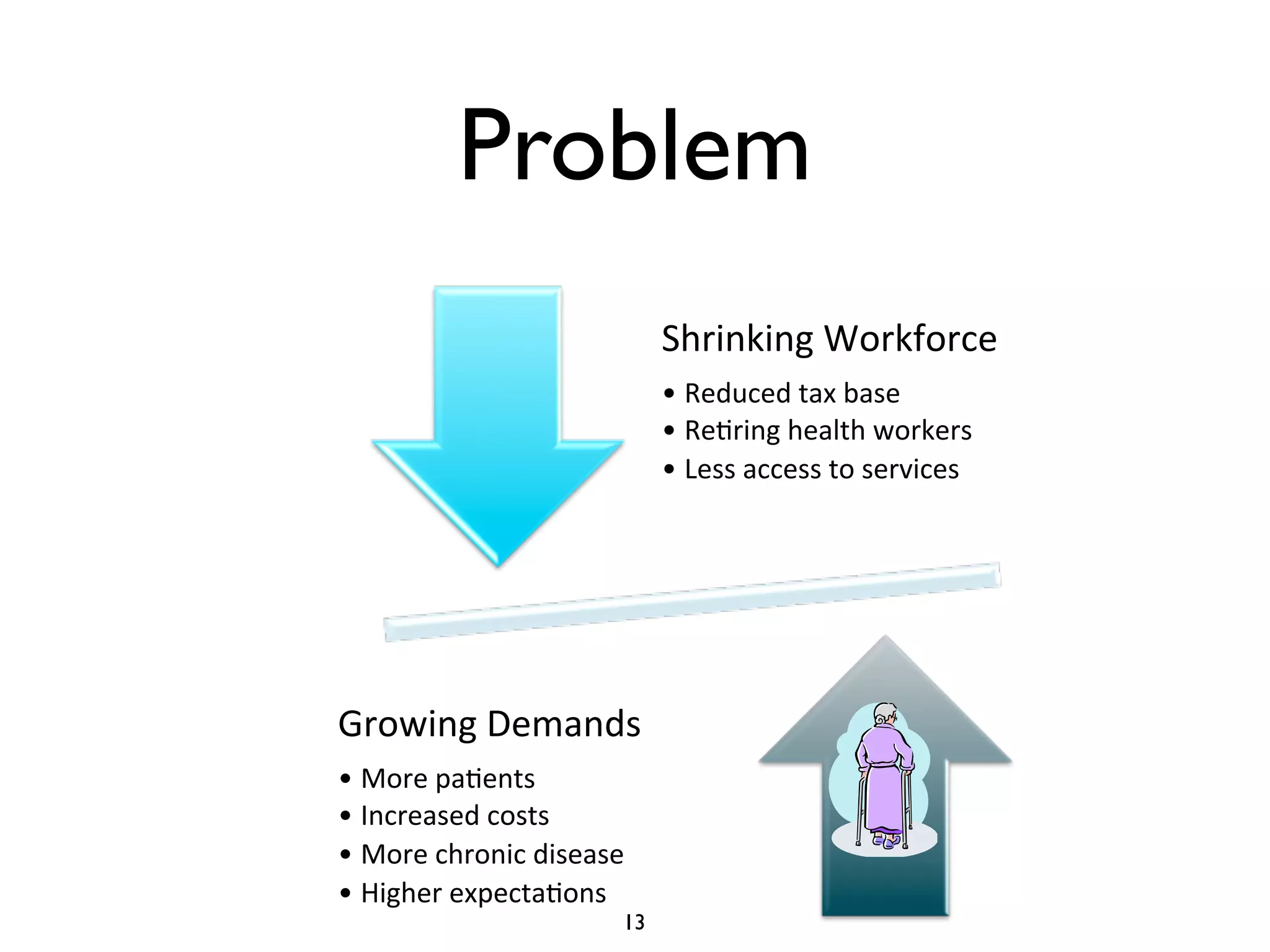
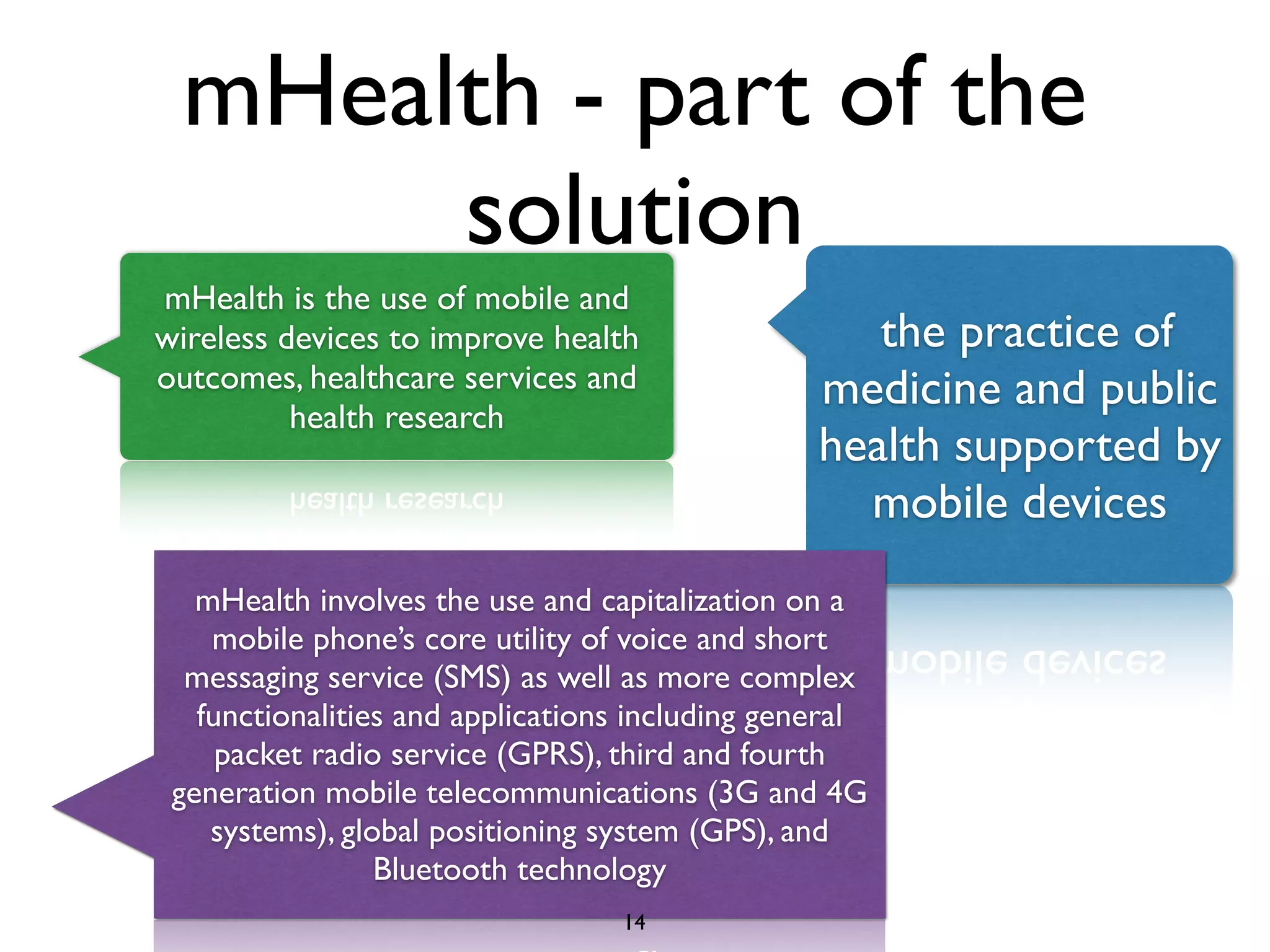
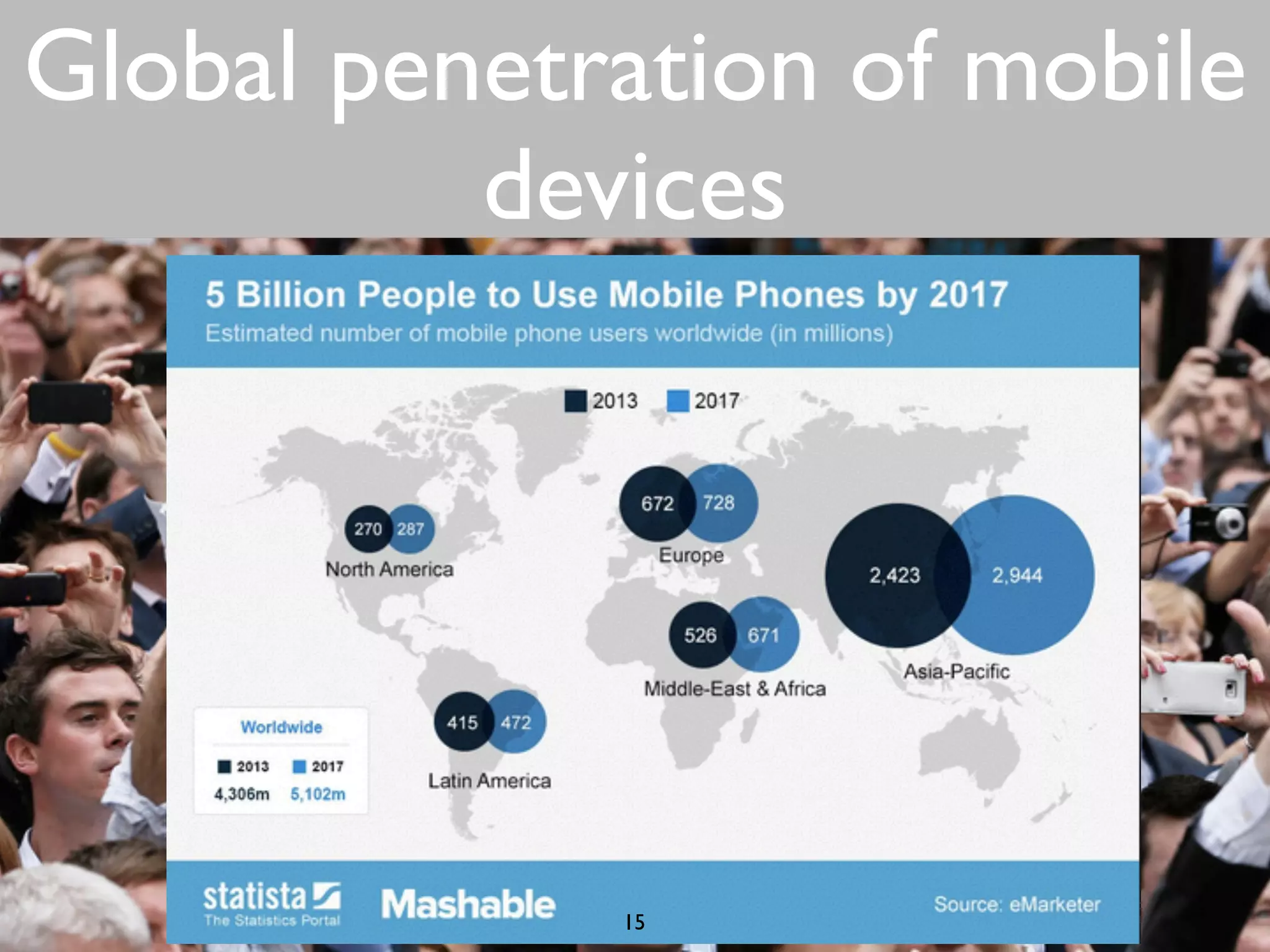
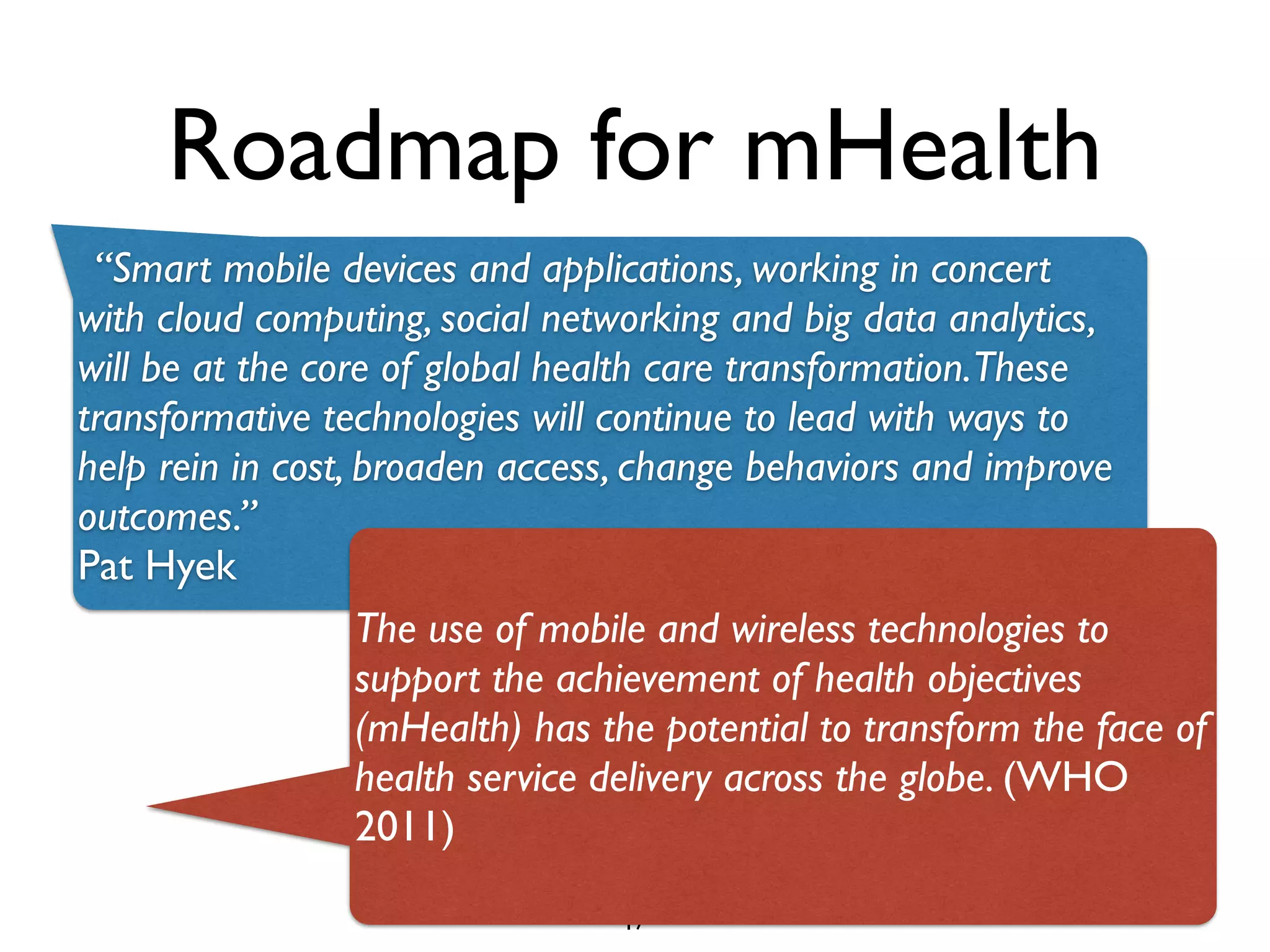
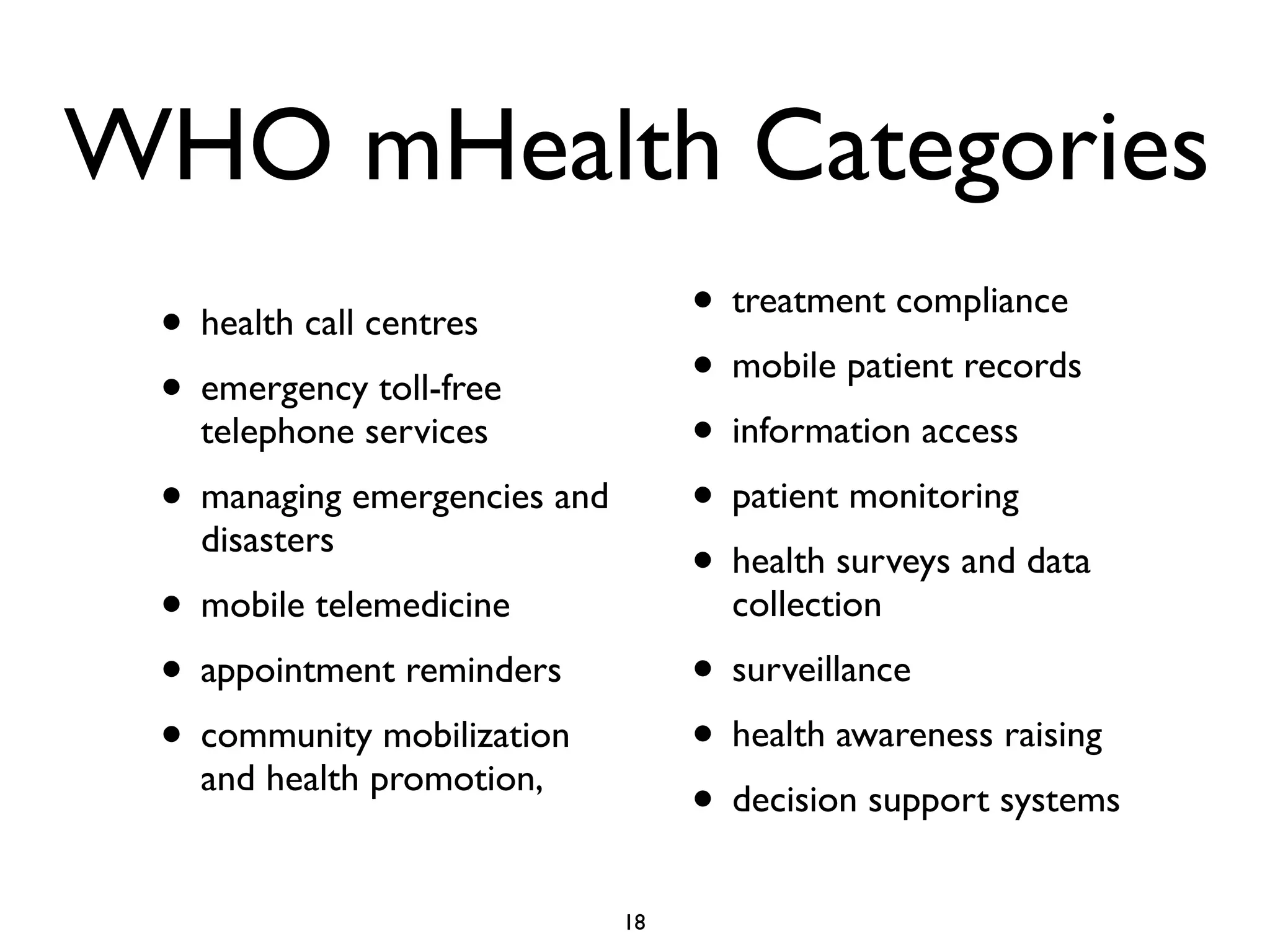
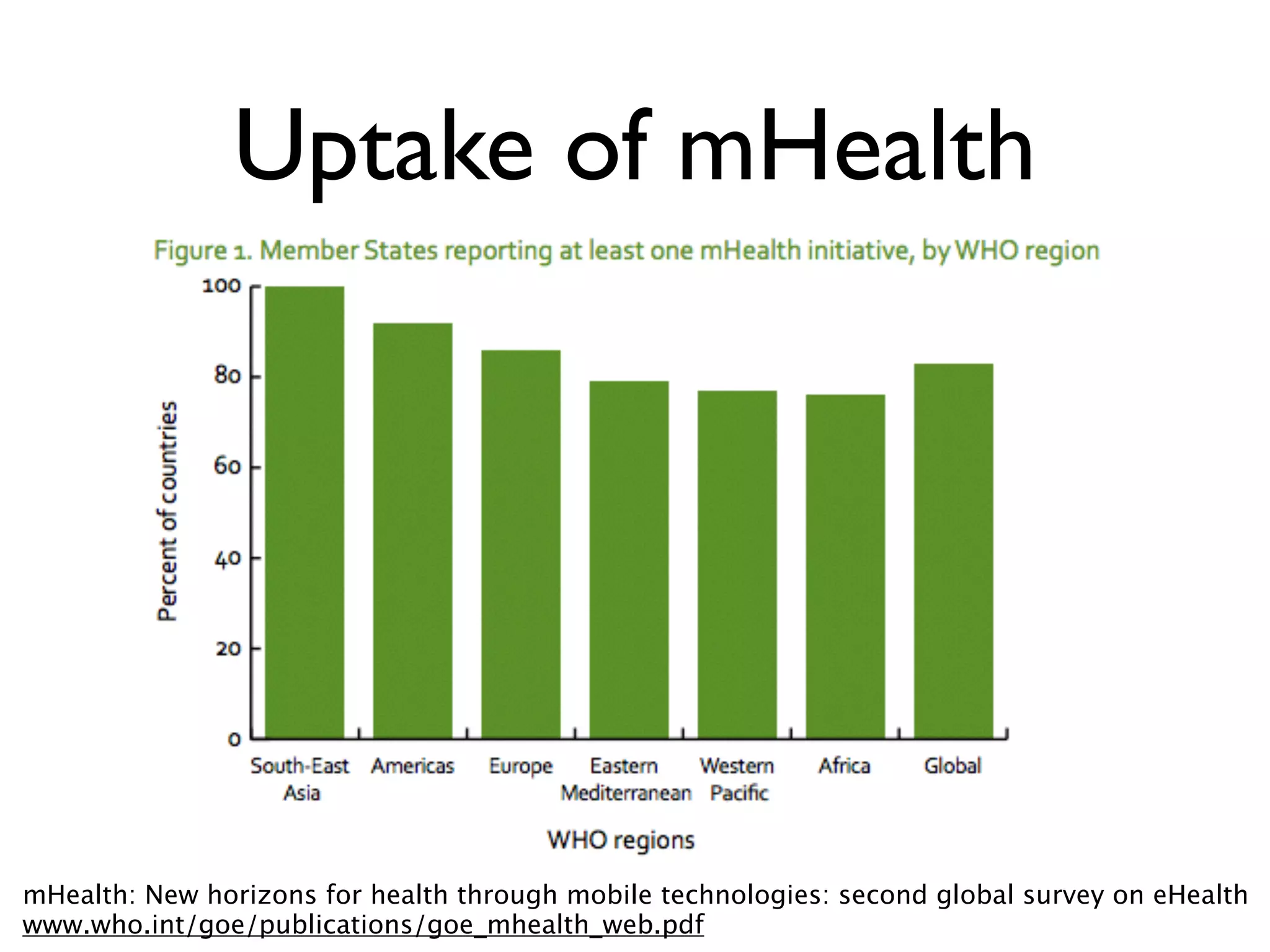
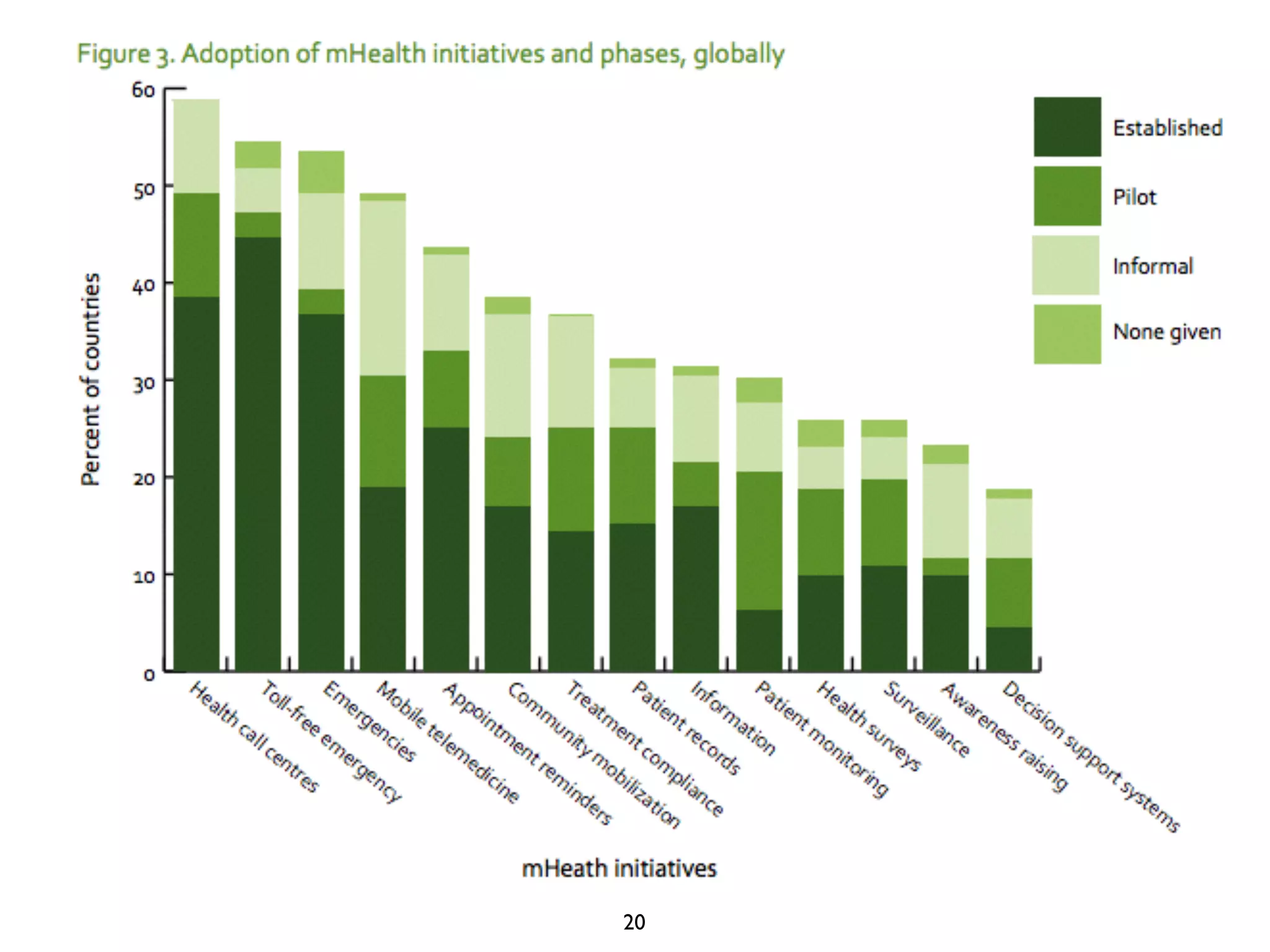
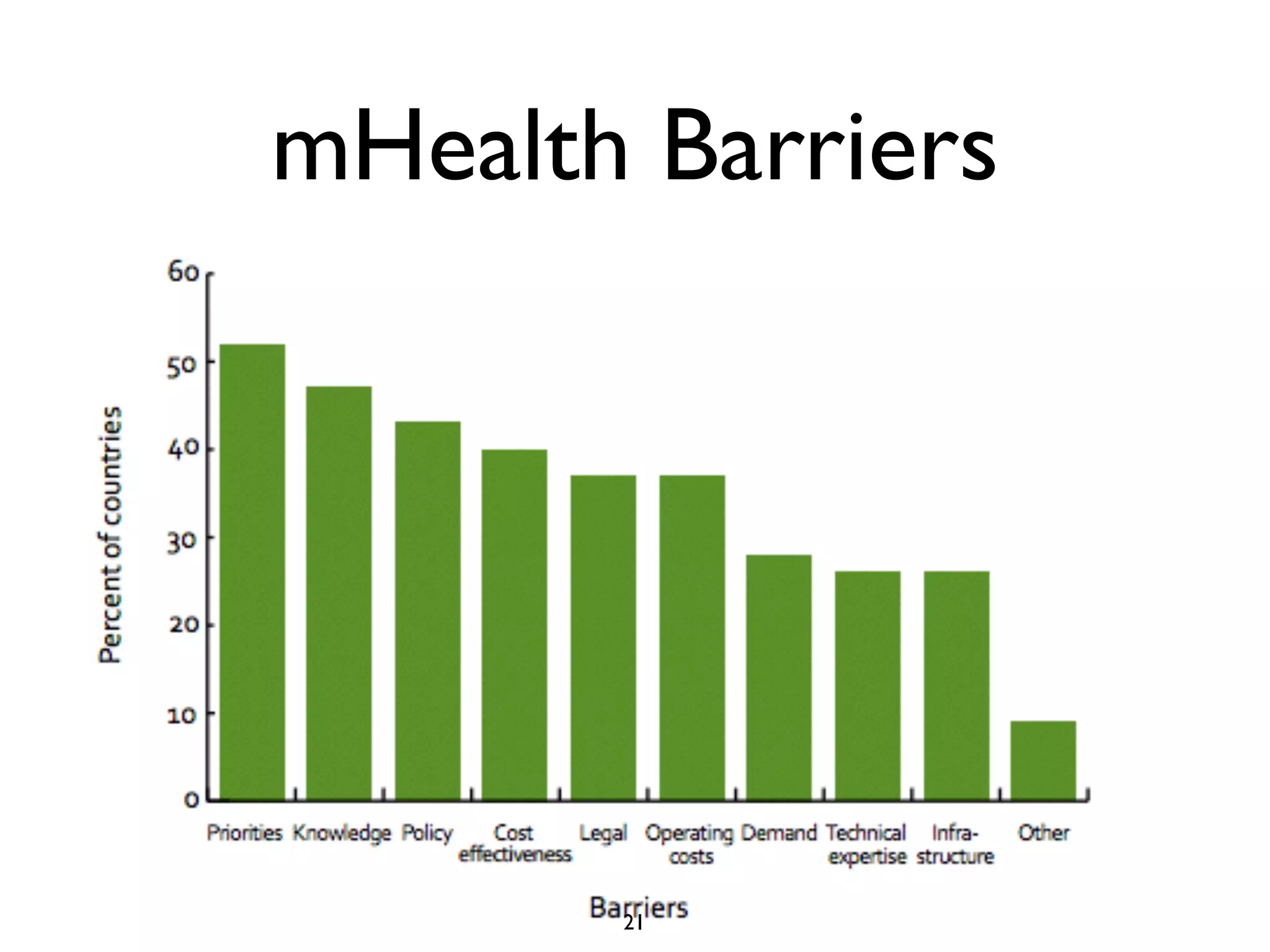
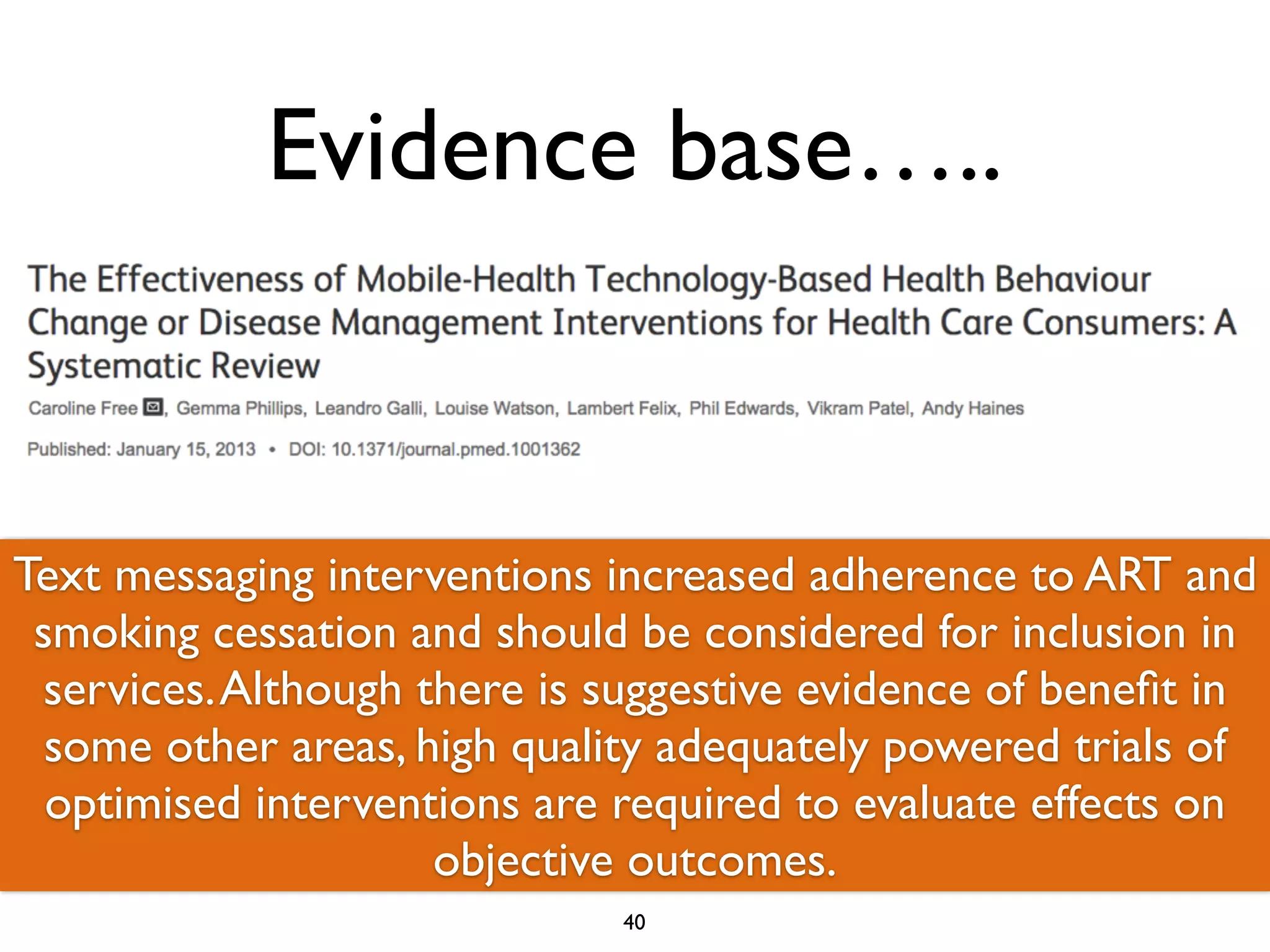
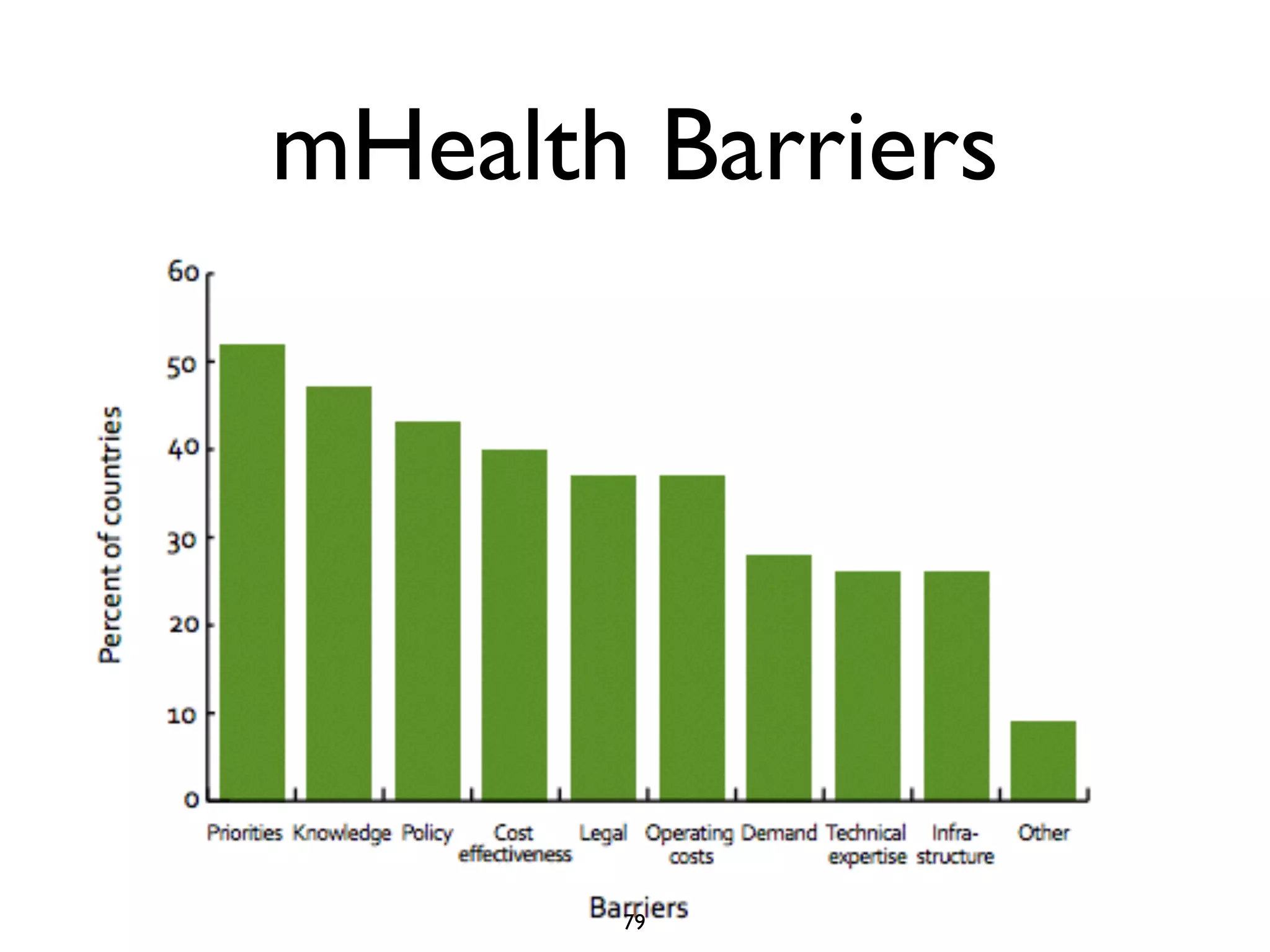
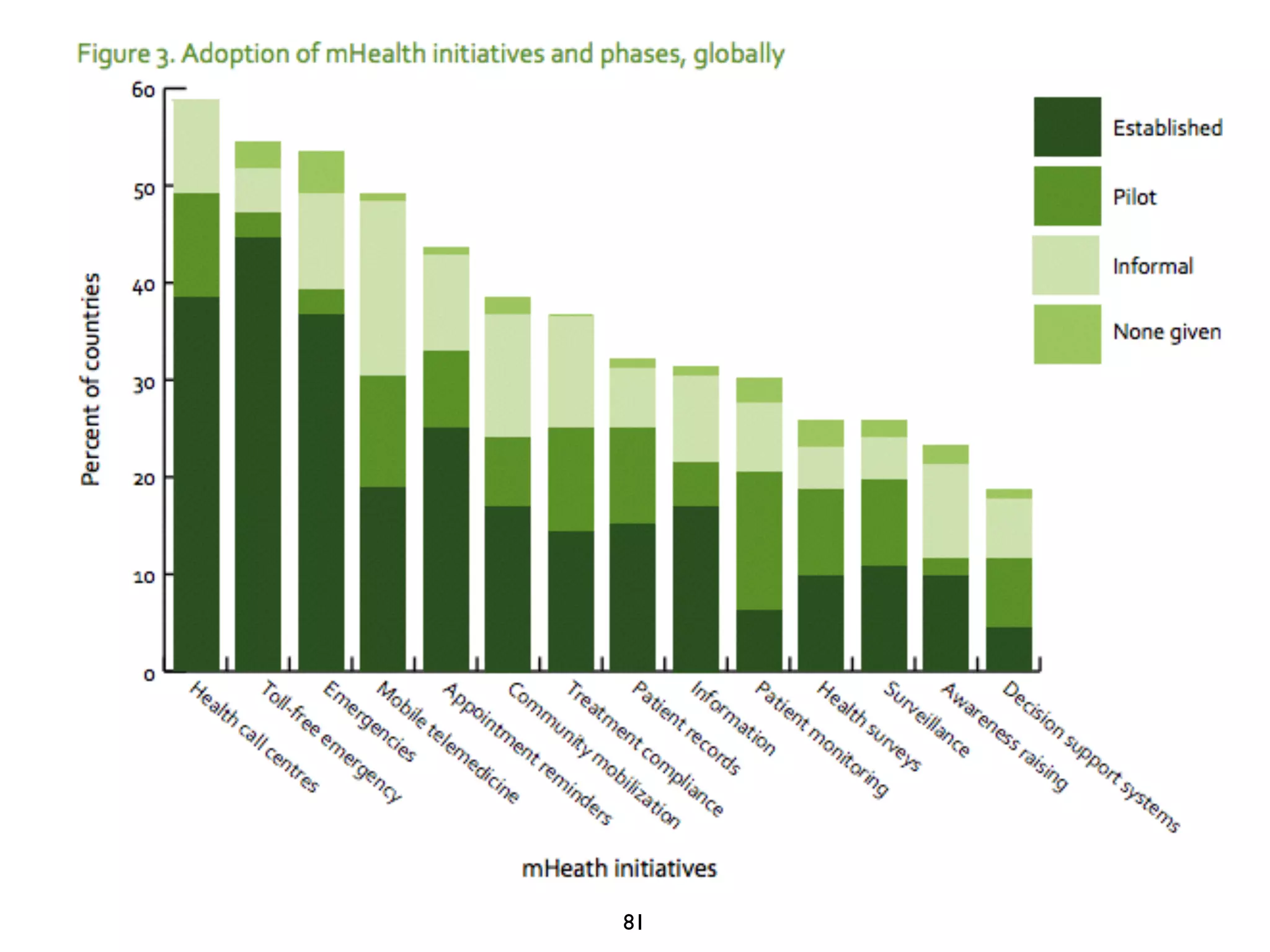
The document discusses the potential of mHealth, which leverages mobile and wireless technology to enhance health outcomes and service delivery globally. It highlights various applications and categories of mHealth, the challenges faced in its implementation, and the importance of rigorous evaluation for the effectiveness of mHealth strategies. The document emphasizes that transformative technologies, such as apps and cloud computing, can help improve health access, reduce costs, and change health behaviors.



































































