Introduction
• Measles (rubeola)is an acute, highly contagious viral disease
characterized by classic features such as high grade fever,
maculopapular rash, cough, coryza and conjunctivitis
• Cause: single-stranded negative sense RNA virus,
Paramyxoviridae family transmitted airborne
• Causes profound immune suppression and amnesia
• Despite vaccine since 1963, it remans a major cause of childhood
morbidity & mortality, especially in developing nations.
4.
Historical Perspective
• 9thcentury: First described by a Persian physician
Rhazes
• Pre-vaccine era: ~2.6 million deaths/year worldwide
• 1963: Live-attenuated vaccine by John Enders &
Thomas Peebles
• Present: Still endemic in Nigeria despite vaccination
efforts
5.
Epidemiology
• 10.3 millioninfections globally in 2023, with ~107,500 deaths
(down from 800,000 in 2000)
• Countries with the highest burden: Yemen, Pakistan, India,
Kyrgyzstan, Afghanistan, Ethiopa, Romania, Nigeria, Canada, and
Russia
• Nigeria (Jan 2025): 627 suspected cases (71% decrease from Jan
2024); 20,000 in 2023, 15,000 in 2020, 30,000 in 2019
• Most affected states: Borno, Katsina, Adamawa, Bayelsa, Ogun,
Oyo
• 73–81% of cases: children ≤2 years
• Case fatality rate: 0.1–0.3% (developed) vs >6% (resource-
limited settings)
6.
Epidemiology…
• Viral Factors:
–Respiratory droplets/aerosols (virus survives 2
hours in air)
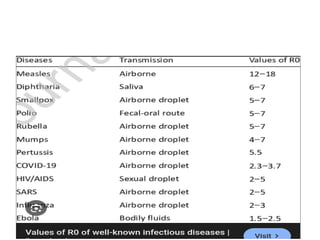
– R :
₀ 12–18 (extremely contagious)
– Incubation: 10–14 days
– Infectious: 4 days before & after rash onset
8.
Epidemiology…
• Host &Environmental Factors
– Age <5 years
– Unvaccinated
– Malnutrition, vitamin A deficiency
– Immunocompromised state
– Overcrowding
– Peak season in Nigeria: January–March (dry
season)
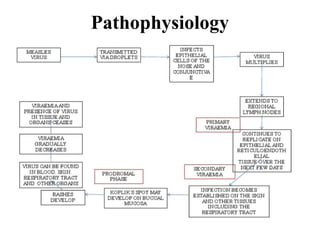
Pathophysiology…
• Entry &primary viremia (days 1–4):
– Virus enters via respiratory tract mucosae, binds
CD150(SLAM) receptors
– Multiplies and spread to regional lymph nodes
– Disseminates into the bloodstream: primary
viremia
12.
Pathophysiology…
• Secondary viremia& systemic spread (days 5–7):
– It gets into the reticuloendothelial tissues and
continues to replicate
– From these tissues, a large amount re-enters the
blood: secondary viremia
– Coincides with prodrome onset
13.
Pathophysiology…
• Immunosuppression &immune amnesia:
– Destruction of T/B cells & memory lymphocytes
– Loss of prior immunity
– Persistence for weeks–months
– Warthin-Finkeldey giant cells formation:
pathognomic
14.
Clinical Features
• Incubationperiod:
– 7-14days after exposure
• Prodromal Phase:
– High grade fever: 39–40°C
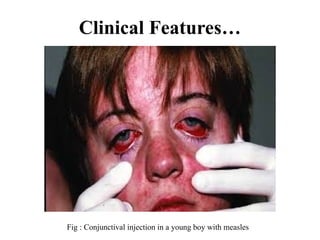
– 3 C's: cough (harsh/brassy), coryza (nasal
discharge), conjunctivitis (red eyes, watery,
photophobia)
– Koplik spots: white or bluish-white spots on
buccal mucosa, appear 1–2 days before rash
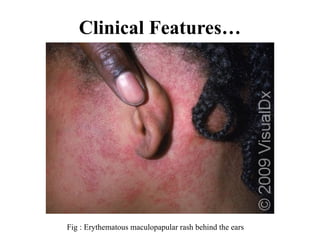
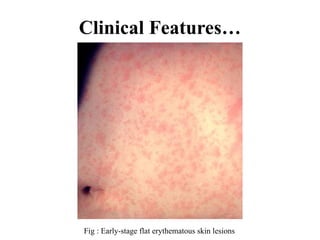
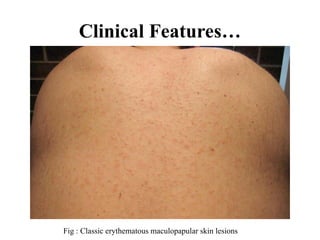
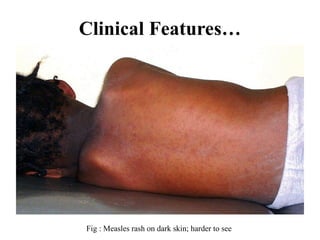
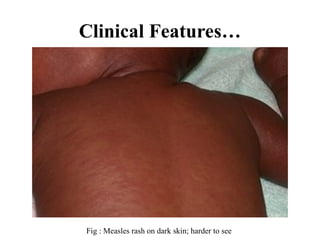
Clinical Features…
• ExanthemPhase:
– Onset: 3–7 days after prodrome
– Head-to-toe spread over 3 days; Day 1: hairline,
behind ears; Day 2: neck, trunk, arms; Day 3:
lower trunk, legs
– Erythematous macules → maculopapular →
confluent on face/trunk, discrete on extremities
• Recovery Phase:
– Resolves in same order; fine desquamation
Treatment
• Supportive:
– Fever:paracetamol/ibuprofen
– Dehydration: ORS, IV fluids
– Nutrition: continued feeding, soft diet
– Oxygen, bronchodilators if needed
32.
Treatment…
• Specific:
– VitaminA: reduces mortality by 50%; <6m:
50,000 IU ×2; 6–12m: 100,000 IU ×2; ≥12m:
200,000 IU ×2
– Antibiotics for bacterial infections
– Isolation: up to 4 days after rash
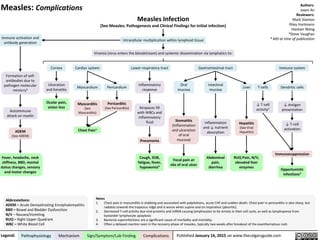
• Complications:
– Treat pneumonia, diarrhea, seizures as needed
33.
Prevention
• Vaccination &PEP
– Monovalent, MR, MMR
– Efficacy: single dose 93–95%, two doses 97%
– Nigerian schedule: 9 & 15 months
– PEP: MMR within 72h; immunoglobulin within 6
days
34.
Prevention…
• Challenges:
– Coveragegaps, geographic barriers, insecurity,
hesitancy, cold chain
– AI tools, integrated health services, mobile teams,
community leader engagement
35.
Conclusion
• Measles remainsa challenge despite interventions
• 71% reduction in Jan 2025 cases shows progress
• >60% complication rate in Nigerian studies
• Vitamin A reduces mortality by 50%
• Need 95% coverage & integrated approach
• Nigeria’s success can guide other countries
36.
References
• Augusta, U.E.,(2016) ‘Common Tropical Viral Infections’, in Azubuike, J.C. &
Nkanginieme, K.E.O. (eds.), Paediatrics and Child Health in a Tropical Region, 3rd
edn. Lagos: Educational Printing and Publishing, pp. 550–552.
• CDC (2024) Measles Videos and Clinical Overviews. CDC Division of Viral
Diseases (multiple entries, including DrDan Filardo’s clinical overview)
Cadmore Media+9CDC+9YouTube+9.
• Dong, T.Q. & Wakefield, J. (2020) ‘Modeling and presentation of vaccination
coverage estimates using data from household surveys’, arXiv preprint
arXiv+1arXiv+1.
• Dong, T.Q. & Wakefield, J. (2020) ‘Space time smoothing models for sub national
‑ ‑
measles routine immunization coverage estimation’, arXiv preprint.
• Filardo, T.(2024) Clinical Overview of Measles: Diagnosis, Laboratory Testing and
Outbreak Response. Webinar hosted by CDC/IDSA/AMA. Published 23 May 2024
EdHub+2CDC+2YouTube+2.
37.
References…
• Filardo, T.(2024)Measles Clinical Presentation, Epidemiology, and Prevention. MeRC
(Measles, Rubella, and CMV) Team, Division of Viral Diseases, National Center for
Immunization and Respiratory Diseases (NCIRD), CDC. Available at: Emory University
Infectious Diseases PDF repository (Accessed: 13 July 2025) UCSF Health
Epidemiology+11Emory School of Medicine+11American Medical Association+11.
• Filardo, T.(2024) Measles: Stories from the Frontlines. CDC/AMA Project Firstline
Forum, 27 June 2024 American Medical Association+2EdHub+2Cadmore Media+2.
• Mathis, A.et al.(2023) ‘We Must Maintain Measles Elimination in the United States:
Measles Clinical Presentation, Diagnosis, and Prevention’, COCA Call, 17August 2023
Cadmore Media+11CDC Stacks+11Infectious Diseases Society of America+11.
• Thakkar, N., Jindal, S. & Rosenfeld, K. (2024) ‘Seasonality and susceptibility from
measles time series’, arXiv preprint arXiv.
• Van den Berg, G.J., von Hinke, S. & Vitt, N. (2023) ‘Early life exposure to measles and
later life outcomes: Evidence from the introduction of a vaccine’,
‑ arXiv preprint arXiv.








































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










