Download as PDF, PPTX


![The centrality of health gain
ISPOR&NEW&ORLEANS IP11
26
21ST
MAY(2019
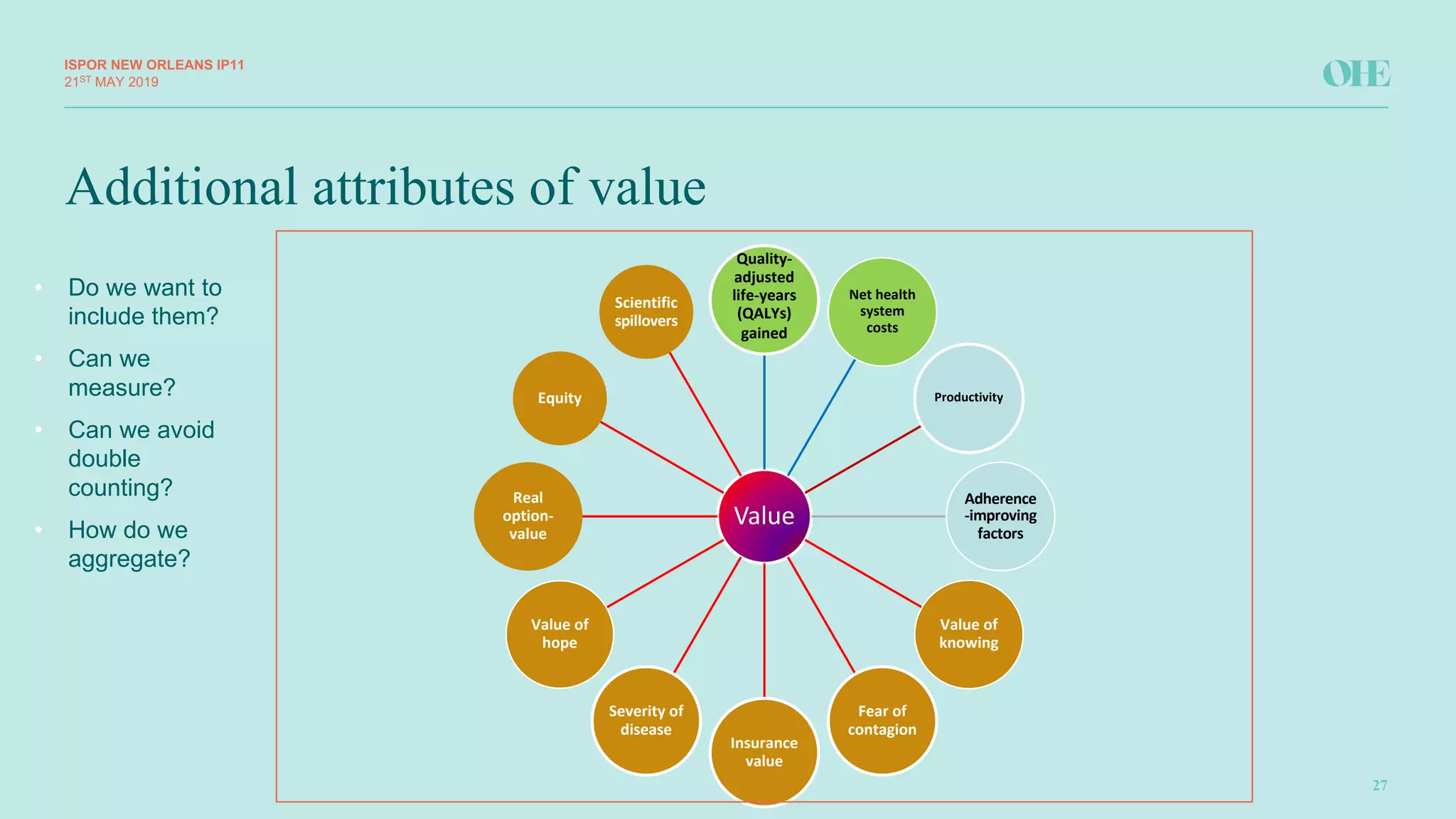
● Assume(it(is(measured(in(QALYs
● A(core(challenge(– can(we(have(things(that(the(health(system(or(an(intervention(provides(that(are(not(to(do(
with(health?(
● The(answer(is(“yes”,(for(example(reassurance,(or(indeed(information(that(is(not(reassuring(but(enables(life(
choices(to(be(made(– the(“value(of(knowing.”(
● But(I(would(argue(it(is(a(key(challenge.(If(it(is(not(an(attribute(that(can(be(expressed(as(a(multiple(of(health(
gain(then(think(carefully.
● This(links(to(a(related(issue.(Even(if(this(“non(health”(attribute(exists(should(the(health(system(be(paying(for(
it?([This(may(also(apply(to(attributes(that(can be(expressed(as(multiples(of(health(gain]
● Again(the(answer(can(be(“yes”(providing(we(are(clear(that(this(is(part(of(the(objectives(of(the(health(
system(to(be(paid(for(in(premiums(P be(they(funded(via(taxes,(social(insurance(or(private(insurance.(
● If(we(have(these(elements(that(are(not(a(function(of(health(gain(and(so(cannot(be(in(a(weighted(QALY(then(
we(can(have(an(estimate(of(Net(Monetary(Benefit((NMB)(or(Net(Health(Effects((NHE),(i.e.(we(can(convert(
them(into($$(or(QALYs(if(we(have(the(relevant(“rate(of(exchange”,(MRS,(or(ʎ](https://image.slidesharecdn.com/mcdadebateispornola2019-190614095952/75/MCDA-OR-WEIGHTED-CEA-BASED-ON-THE-QALY-WHICH-IS-THE-FUTURE-FOR-HTA-DECISION-MAKING-26-2048.jpg)

The document discusses the evolving methodologies in health technology assessment (HTA), focusing on the potential integration of augmented cost-effectiveness analysis (CEA) and multi-criteria decision analysis (MCDA). It emphasizes the limitations of traditional CEA in addressing complex decision-making factors, advocating for structured approaches that consider multiple dimensions of value. The presentation aims to explore the merits of augmented CEA and MCDA, highlighting the importance of transparency and improved decision-making processes in health care.






































































