
Download to read offline


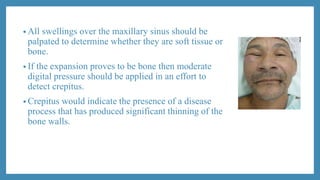
![MAXILLARY SINUS
[EXAMINATION ,RADIOGRAPHIC
INVESTIGATION AND PATHOLOIES ]
PRESENTED BY –ZAREESH .S.AKHTAR
1 MDS IN ORAL MEDICINE AND RADIOLOGY](https://image.slidesharecdn.com/maxillarysinuspart2-210925165256/85/Maxillary-sinus-part-2-2-320.jpg)
![RADIOGRAPHIC INVESTIGATION OF MAXILLARY
SINUS
Extraoral views
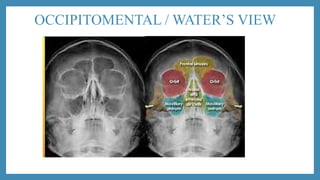
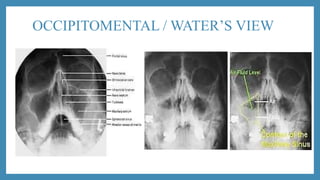
• Occipitomental / water’s view
• Lateral cephalometry [lateral
skull ]view
• Submentovertex view
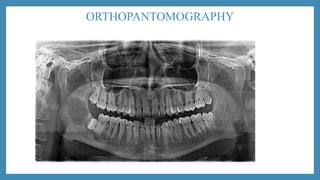
• Orthopantomography
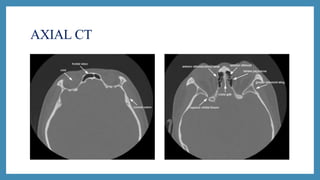
• CT scan
• MRI
Intraoral view
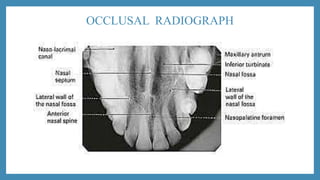
• Occlusal
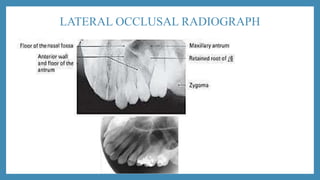
• Lateral occlusal
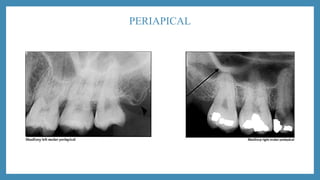
• Periapical](https://image.slidesharecdn.com/maxillarysinuspart2-210925165256/85/Maxillary-sinus-part-2-15-320.jpg)
![LATERAL CEPHALOMETRY [LATERAL SKULL ]VIEW](https://image.slidesharecdn.com/maxillarysinuspart2-210925165256/85/Maxillary-sinus-part-2-21-320.jpg)

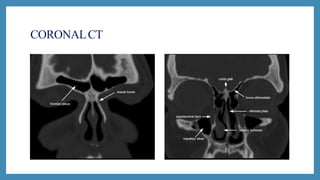
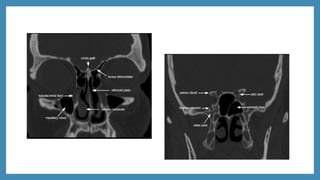
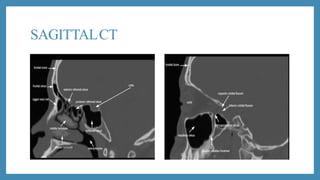
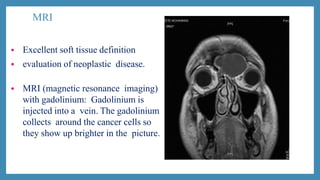
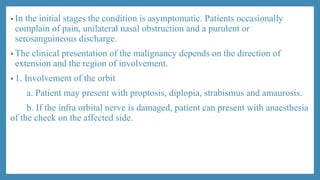

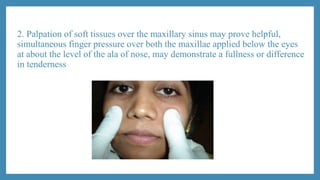
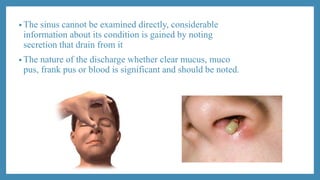
The document discusses examination, radiographic investigation, and pathologies of the maxillary sinus. Examination involves extraoral and intraoral inspection and palpation to check for tenderness, swelling, or discharge from the sinus. Radiographic views like panoramic x-ray, CT scan, and MRI provide images of the sinus. Common pathologies include sinusitis (acute, chronic), cysts, tumors, trauma like fractures, and systemic diseases affecting the sinus.
















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





