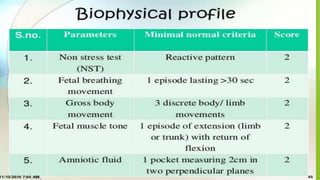
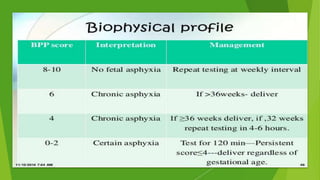
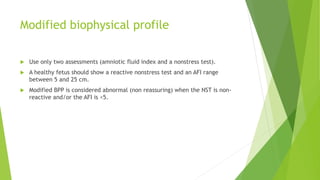
The document provides information on various methods used to assess maternal and fetal wellbeing during pregnancy. The goals of antenatal assessment are to ensure fetal growth and detect any risks affecting the fetus. Methods discussed include maternal serum screening tests, amniocentesis, biophysical profile monitoring, ultrasonography, and Doppler studies. Together these non-invasive and minimally invasive tests can evaluate fetal growth, check for abnormalities, and detect any signs of fetal distress.