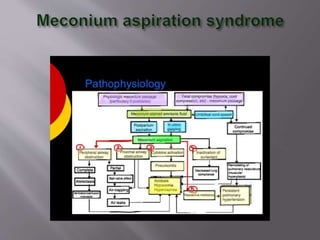
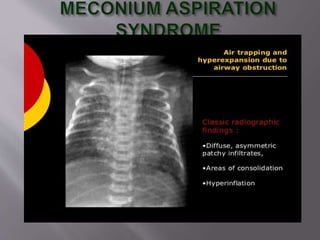
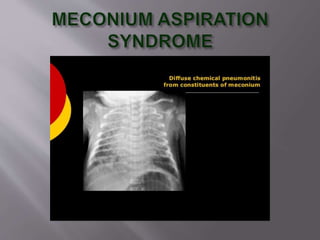
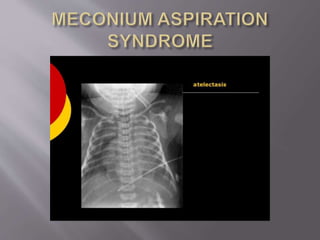
Meconium aspiration syndrome is caused by inhalation of meconium during delivery, which can lead to respiratory distress. Risk factors include post-term pregnancy, fetal stress, and maternal complications. Affected infants may experience cyanosis, grunting, and respiratory distress. Treatment involves suctioning meconium, supportive care, antibiotics, and potentially mechanical ventilation. While most recover fully, severe cases are associated with long-term pulmonary and neurological complications.


































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)








