Downloaded 19 times


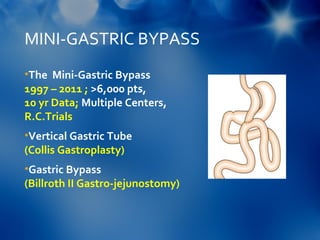
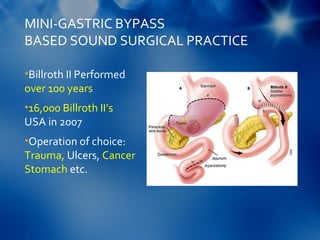
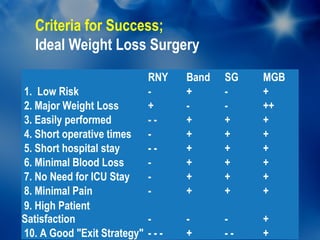
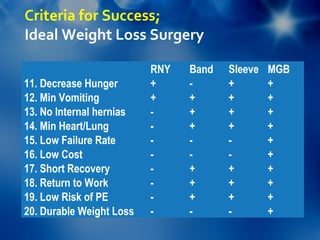
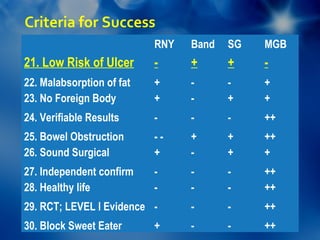


The document discusses the first international consensus conference on mini-bypass surgery, highlighting success criteria for 'ideal' weight loss surgery and the advantages of mini-gastric bypass (MGB) over other procedures. It details the incidence of marginal ulcers as a common postoperative complication and emphasizes the importance of vigilant management to prevent them. The conclusion suggests that MGB best meets the objectives of effective weight loss surgery while being cautious of marginal ulcers associated with Roux-en-Y gastric bypass.