Download to read offline


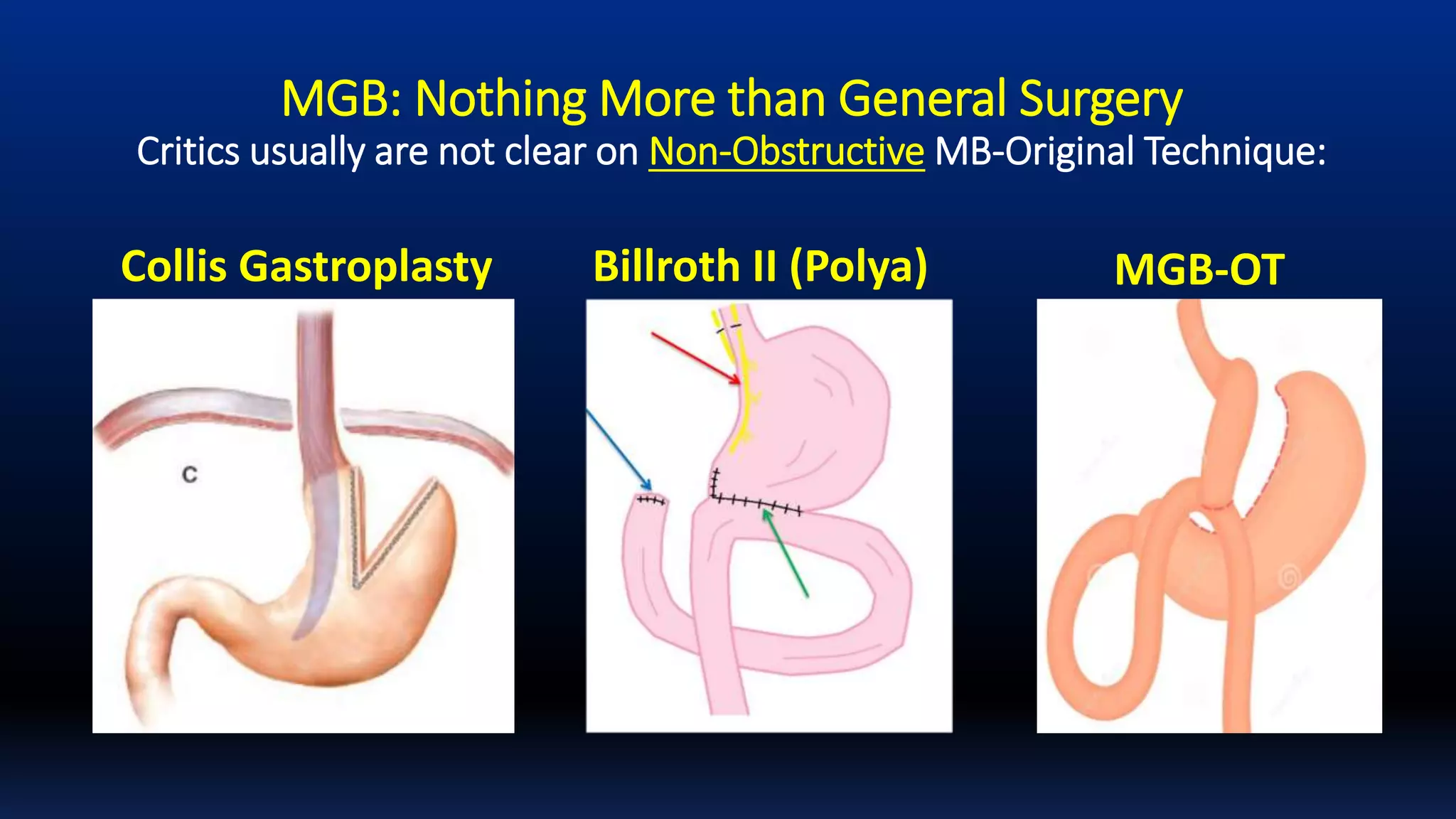





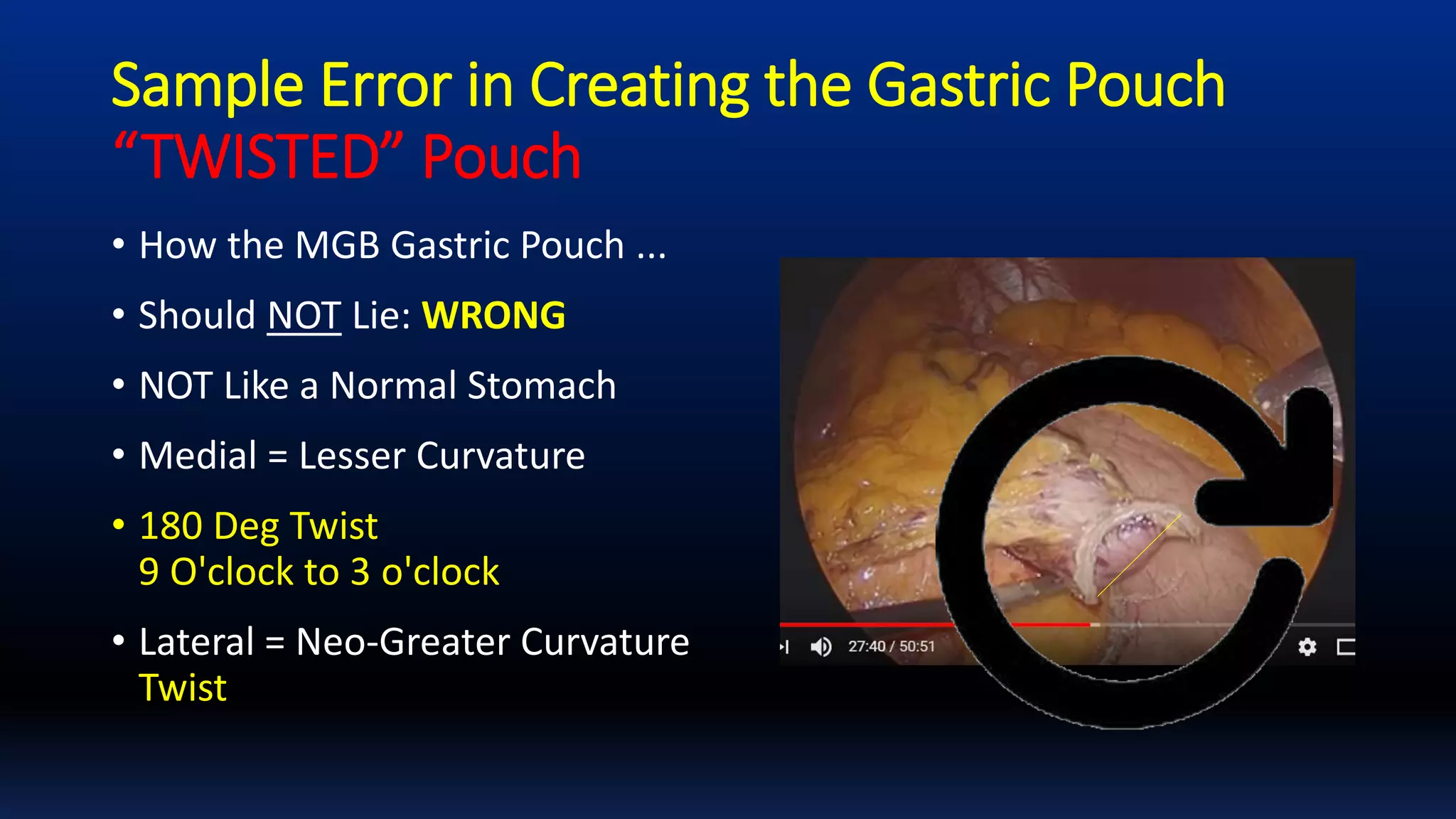


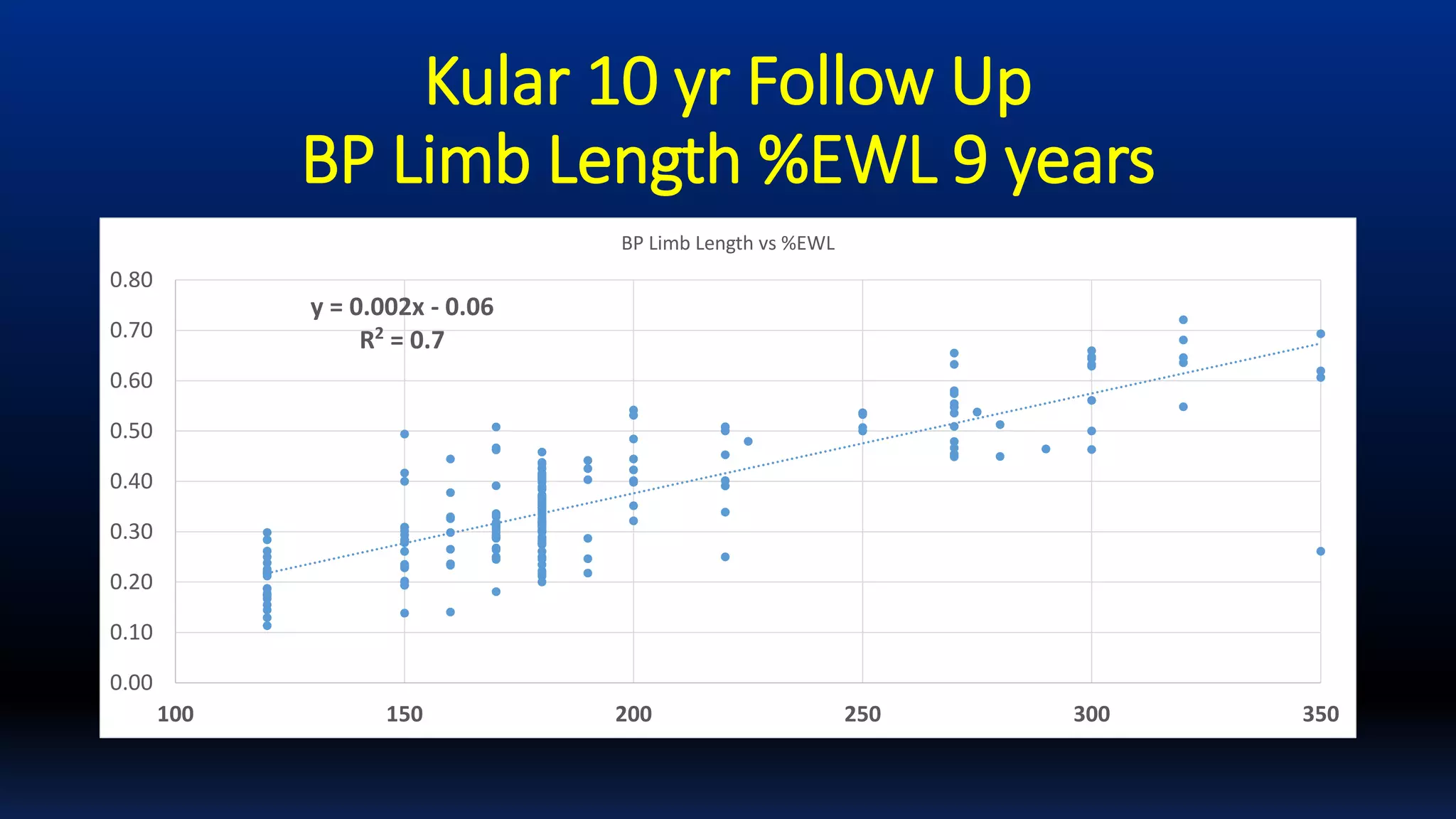


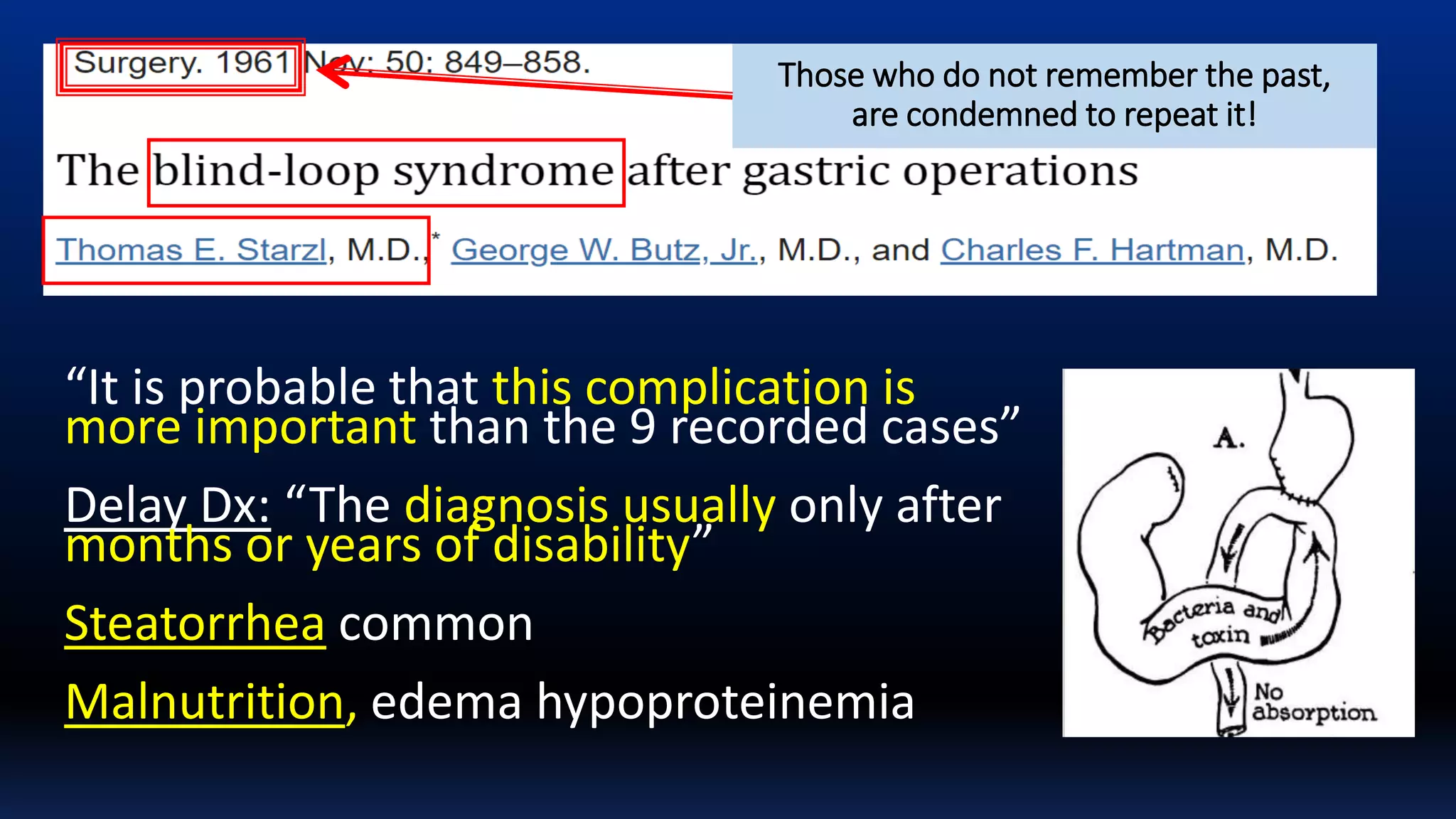
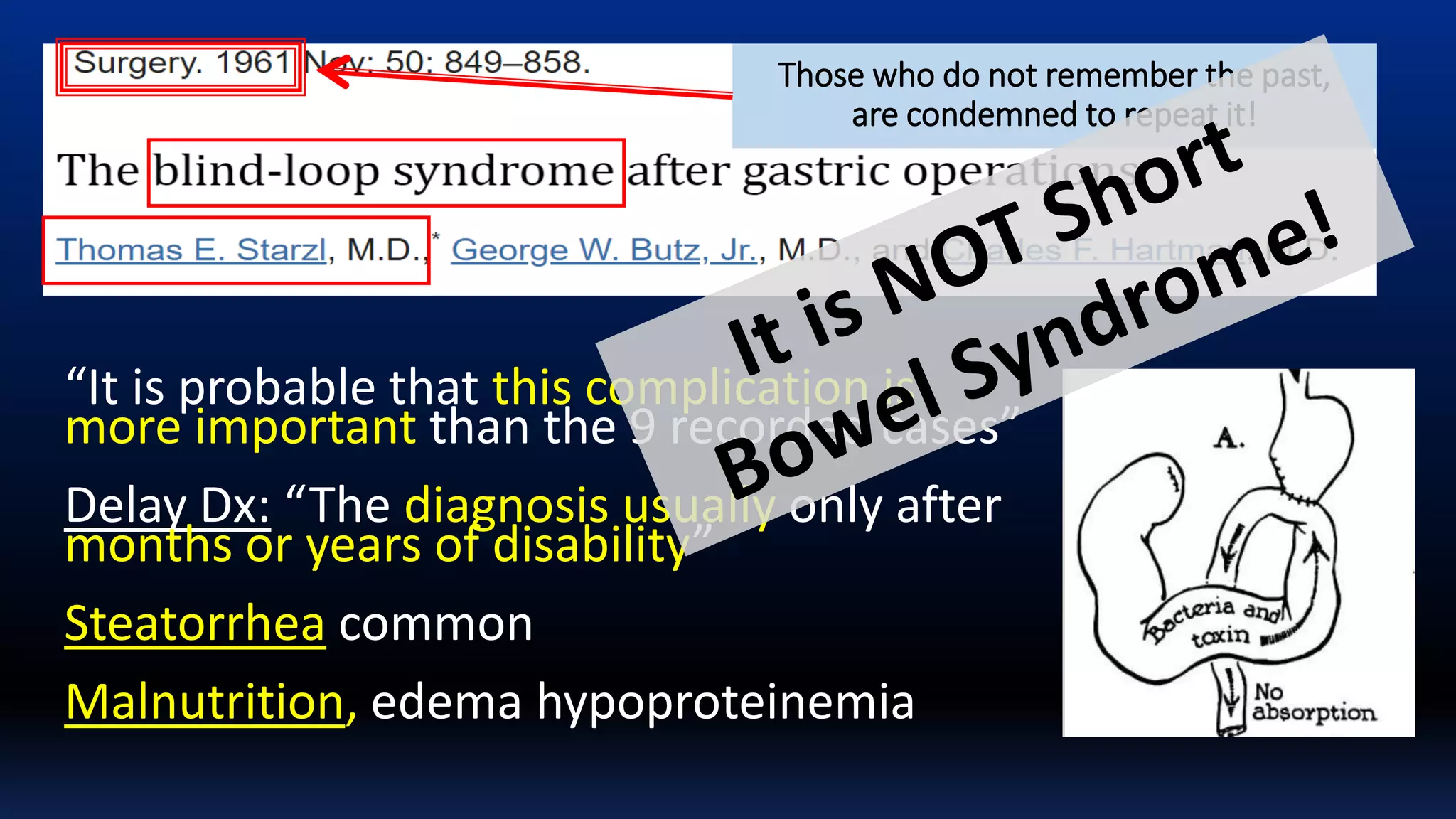
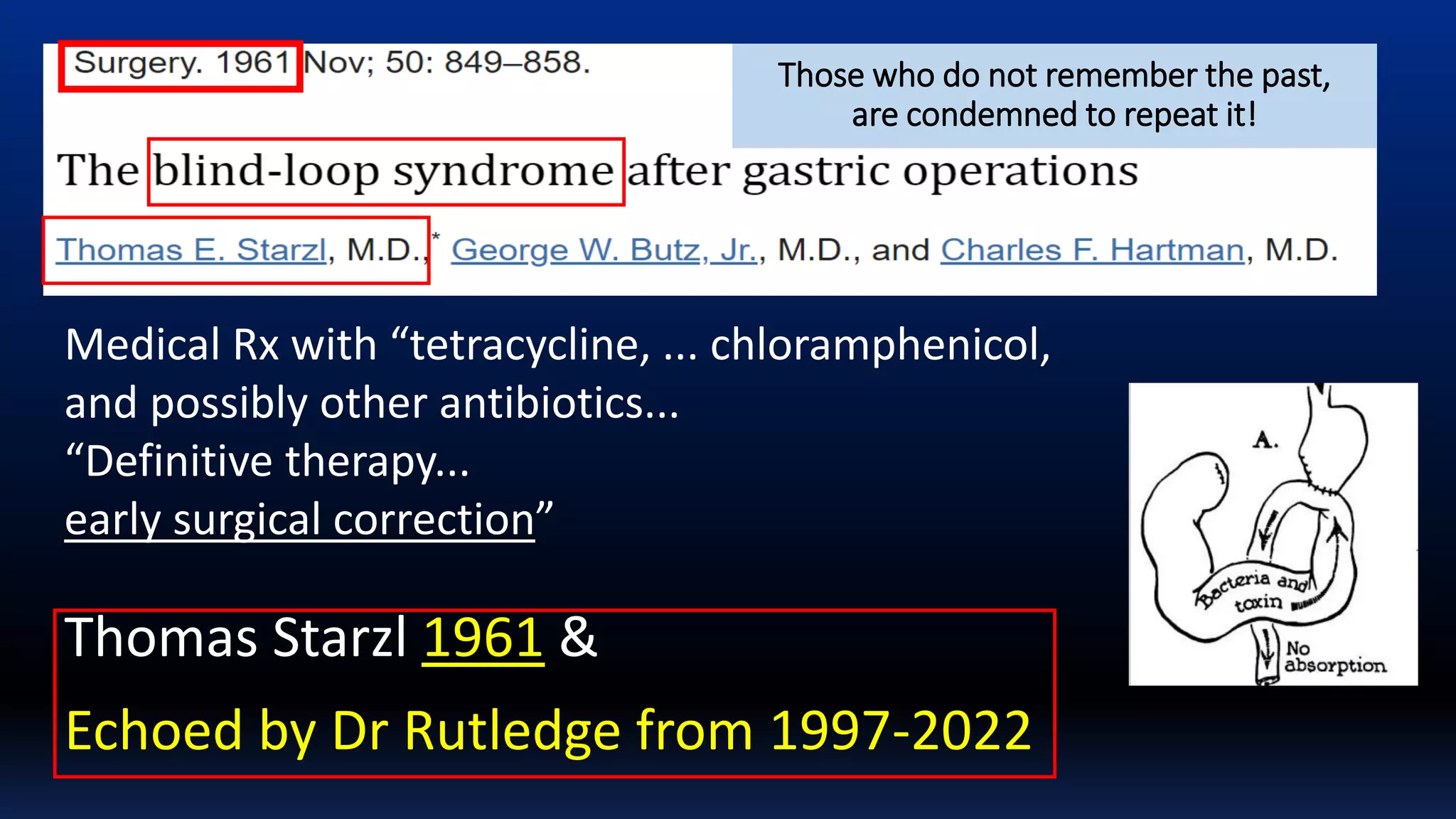



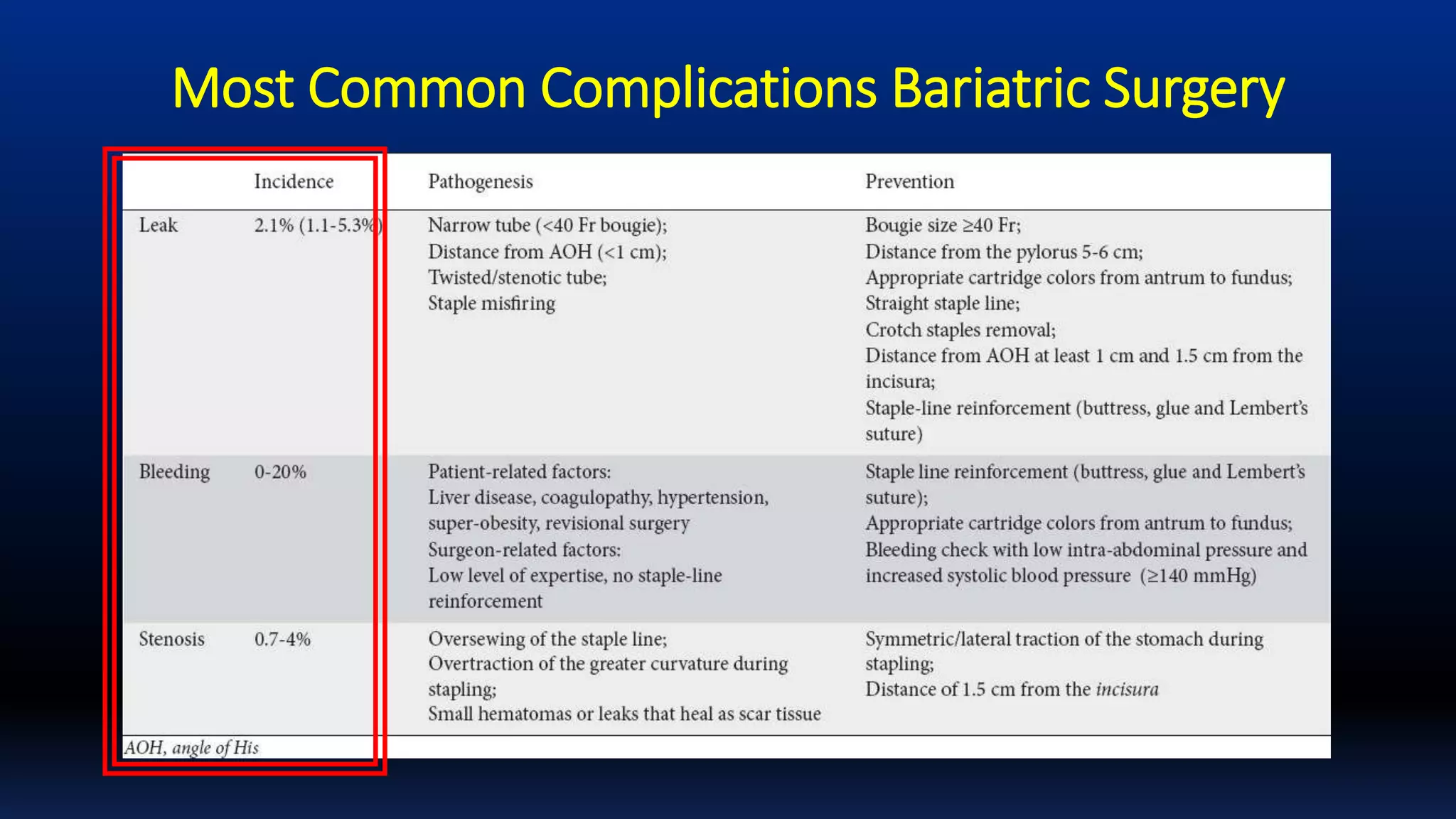







The document discusses the mini-gastric bypass (MGB) technique, its mechanisms, and the controversies surrounding its efficacy and outcomes. It contrasts excellent results reported by some surgeons with complications and failures attributed to poor surgical technique and patient management. Additionally, the document explores the impact of bypass limb length and addresses the importance of understanding postoperative management, malabsorption, and potential complications.

































































