Download to read offline
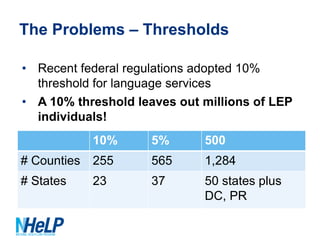
The document discusses language access requirements under the Affordable Care Act (ACA) and opportunities and challenges for enrolling limited English proficient (LEP) individuals in health insurance exchanges. It notes that 23% of expected exchange applicants speak a language other than English and that 95% of uninsured LEP individuals will be eligible for financial assistance. While the ACA includes nondiscrimination protections and data collection requirements to support LEP individuals, some federal regulations have adopted a 10% language threshold that excludes many needed translations. Stakeholders are urged to get involved now to ensure exchanges are designed to effectively enroll and service LEP populations.