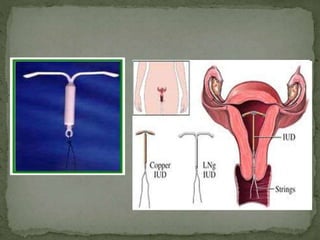
This document provides an overview of long-acting reversible contraceptives (LARCs). It discusses that LARCs include intrauterine devices, implants, and injectables that are effective for 1-5 years. While effective at preventing pregnancy, LARCs have low usage rates due to lack of access and awareness as well as misperceptions about safety. The document reviews the various LARC methods, including types like intrauterine devices, implants, and injectables. It discusses their mechanisms of action, effectiveness, benefits, and risks to provide clinicians with information to educate women about LARC options for pregnancy prevention.

![[Levonorgestrel Implant]
1st generation of implants
Consists of 6 rods, each measuring 34mm in length &
2.4mm in diameter](https://image.slidesharecdn.com/longactinghormonalcontraceptives-150605151233-lva1-app6892/85/Long-acting-hormonal-contraceptives-32-320.jpg)
![JADELLE [NORPLANT-2]
Levonorgestrel preparation
Contains 2 non-biodegradeable silicone elastomer
capsule.
Each capsule is 43mm in length & 2.5mm in diameter.
Each capsule contains 75mg Levonorgestrel.
Insertion is effective for 5yrs.](https://image.slidesharecdn.com/longactinghormonalcontraceptives-150605151233-lva1-app6892/85/Long-acting-hormonal-contraceptives-36-320.jpg)