Case 1 :Tapelo
5- year-old preschool aged girl
Became ill within the last 6 hours
Severe sore throat
Muffled voice
Drooling of saliva
22/01/2022 URI LECTURE 2
Diagnosis: Acute Epiglotittis
DONOT:
Examine the throat
Try to get IV access or bloods
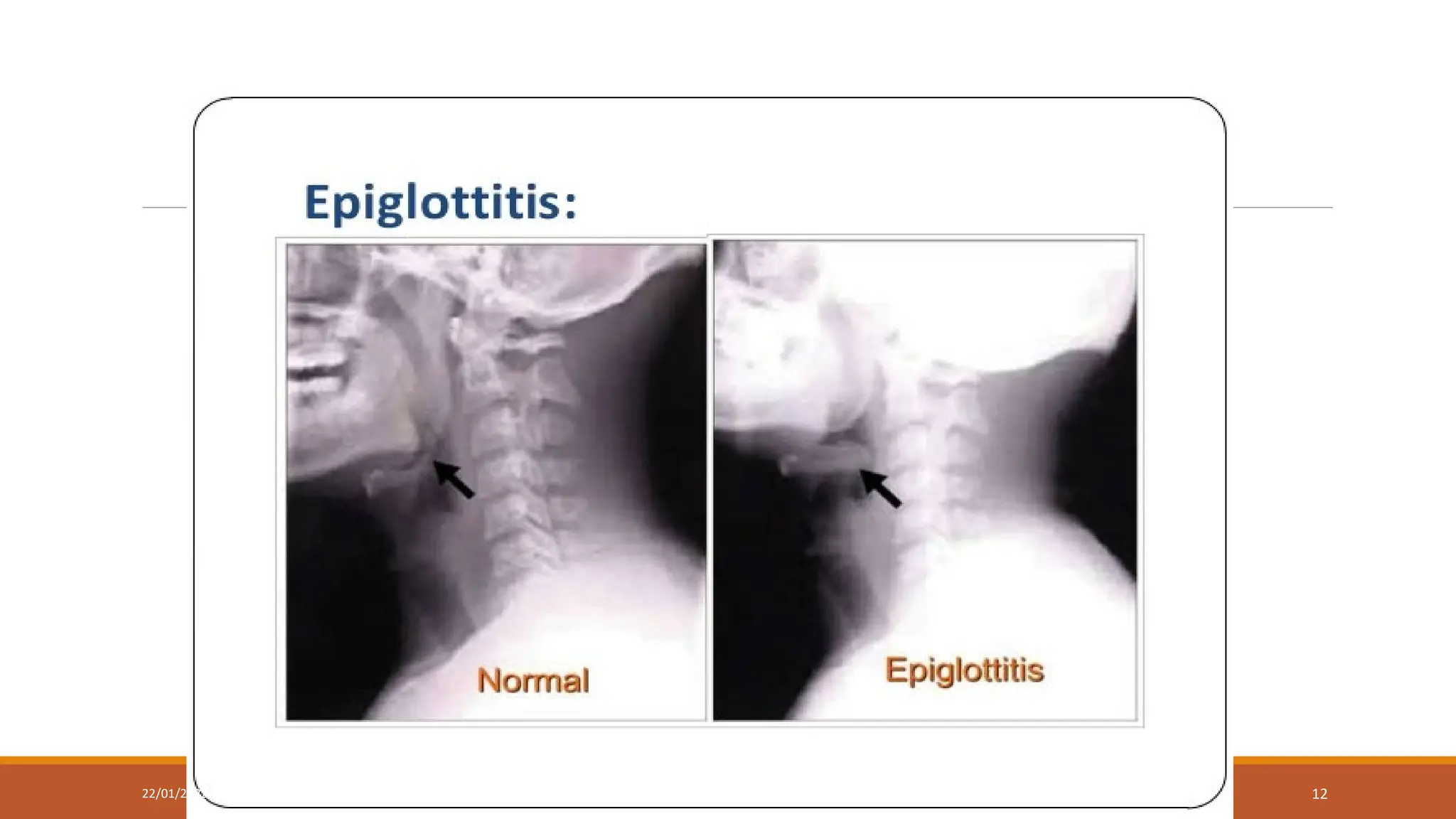
Order lateral neck X-ray
DO:
Summon:
Paediatrician
ENT Surgeon
Anaesthetist
22/01/2022 URI LECTURE 5
Acute Epiglottitis
Caused byH. influenzae type B
The incidence has reduced by 99% due to Hib vaccine
Most common age group is 1-6 years
22/01/2022 URI LECTURE 8
9.
Clinical presentation ofEpiglottitis
There is sudden onset of sore throat, drooling, odynophagia or dysphagia
Muffled dysphonia or loss of voice
Dry cough or no cough
22/01/2022 URI LECTURE 9
Case 2: Mutinta
3-year-old female toddler
Unwell for one day
Sudden onset of sore throat
No cough
Fever
Difficulty feeding
Vomiting
Abdominal pain
22/01/2022 URI LECTURE 14
15.
On examination
Pulse rate:140 beats/minute
Respiratory rate: 40 breaths/minute
Temperatureof 39oC
Tender anterior cervical lymph nodes
Erythematous pharynx with enlarged tonsils and yellowish exudate
22/01/2022 URI LECTURE 15
Diagnosis: Pharyngotonsillitis
PLAN
Admit toward
IV access
Crystalline Penicillin 50 000 IU/kg/dose QID IV
Maintenance IV fluids: Half strength darrows in 10 % dextrose
Paracetamol 15 mg/kg/dose
FBC/DC
22/01/2022 URI LECTURE 17
18.
22/01/2022 URI LECTURE18
If the child has a weight of 20 kg, and continues to
refuse food, how much sour milk could you give the
child every 3 hours by nasogastric tube?
19.
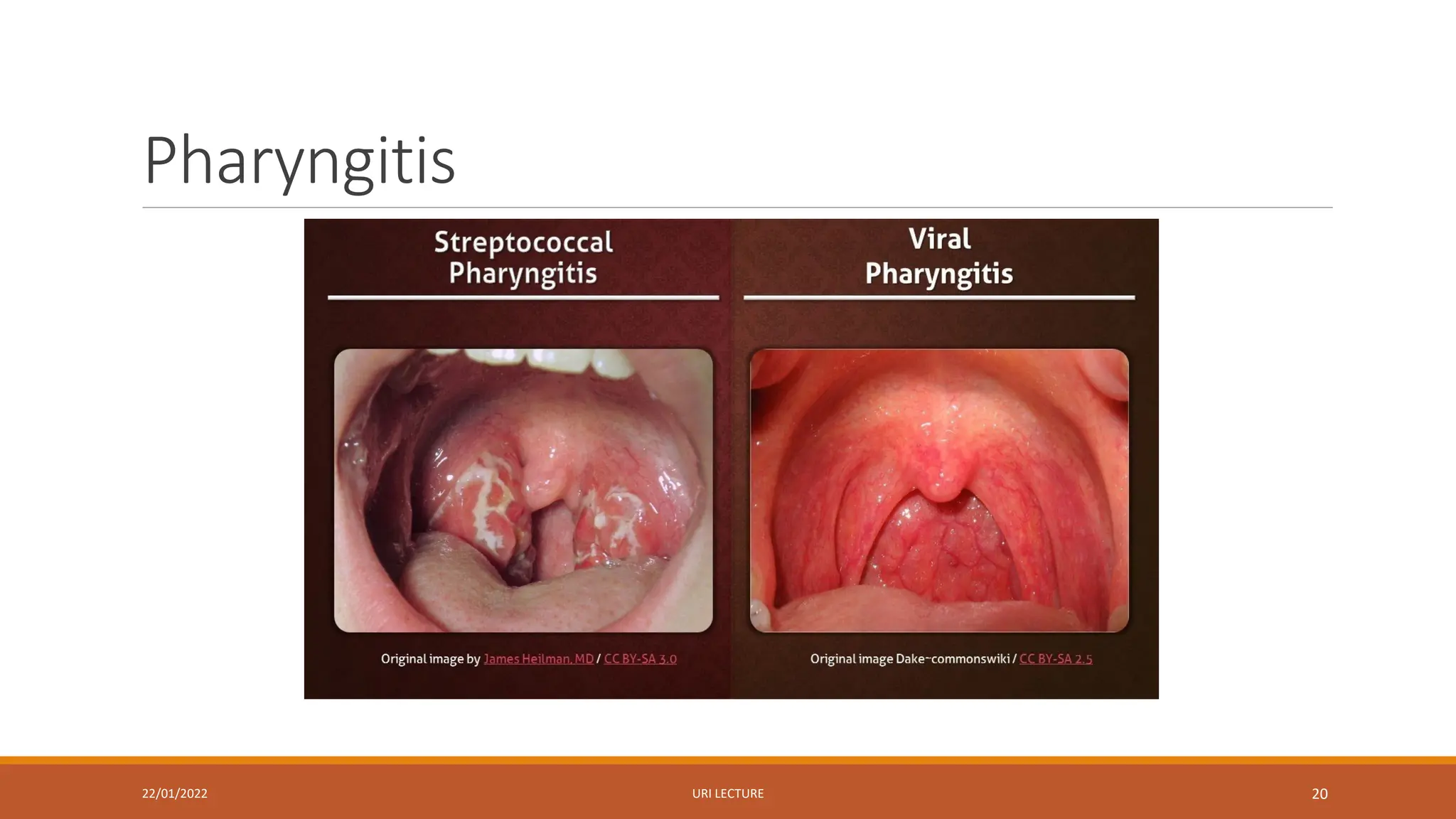
Pharyngitis
It is mostlycaused by viruses and Group A β haemolytic streptococcus
The onset of streptococcal pharyngitis is sudden with prominent sore throat and
fever and absence of cough and rhinorrhoea
The pharynx is red, the tonsils are enlarged and covered with a yellow blood
tinged exudate
22/01/2022 URI LECTURE 19
Clinical Manifestations ofPharyngitis
The soft palate may have petechiae and the uvula may be inflamed as well
The anterior cervical lymph nodes are enlarged and tender
The onset of viral pharyngitis is more gradual and characterised bycoryza,
conjunctivitis, hoarseness and cough
The aim of specific diagnosis is to identify Group A β haemolytic streptococcus
22/01/2022 URI LECTURE 21
22.
Treatment of Pharyngitis
Phenoxymethylpenicillinorally 250 mg every 12 hours for 10 days in children
weighing less than 27 kg
Phenoxymethylpenicillin orally 500 mg every 12 hours for 10 days in children
weighing >27 kg
Benzathine penicillin given IM as a singular dose can be used as well in a hospital
setting: 1.2 MU in children > 27 kg and 600 000 IU in children < 27 kg
22/01/2022 URI LECTURE 22
Indications for Tonsillectomy
Morethan 7 episodes in the previous year
More than 5 in each of the preceding 2 years
Peritonsillar abscess
22/01/2022 URI LECTURE 24
25.
Case 3: Kalonga
2-year-oldtoddler
1 day history of barking cough and fever
Coryzal symptoms
Noisy breathing
SOB
22/01/2022 URI LECTURE 25
26.
On examination
Alert
Temp 38oC
Hoarsenessof voice
Barking cough
Harsh inspiratory stridor
Sub-costal recessions
Transmitted sounds on auscultation
22/01/2022 URI LECTURE 26
Diagnosis: Viral Croup
PLAN
DexamethasonePO 600mcg/kg
Budesonide 2 mg nebulized if vomiting
Observe
Discharge if mild to moderate croup
For severe croup
Adrenaline 1: 1000 neb 5mls
Anaesthetist assessment
May need intubation and ventilation
22/01/2022 URI LECTURE 28
29.
Laryngotracheobronchitis (Croup)
It ismostly caused by viruses
80% are caused by Parainfluenza viruses (1,2 or 3)
It causes upper airway obstruction
These signs are preceded by a low grade fever,rhinorrhea, cough and
pharyngitis
22/01/2022 URI LECTURE 29
30.
Clinical Manifestations ofLTB
Barking cough
Hoarseness
Stridor
High fevers
Hypoxia and low oxygen saturations are rare
22/01/2022 URI LECTURE 30
31.
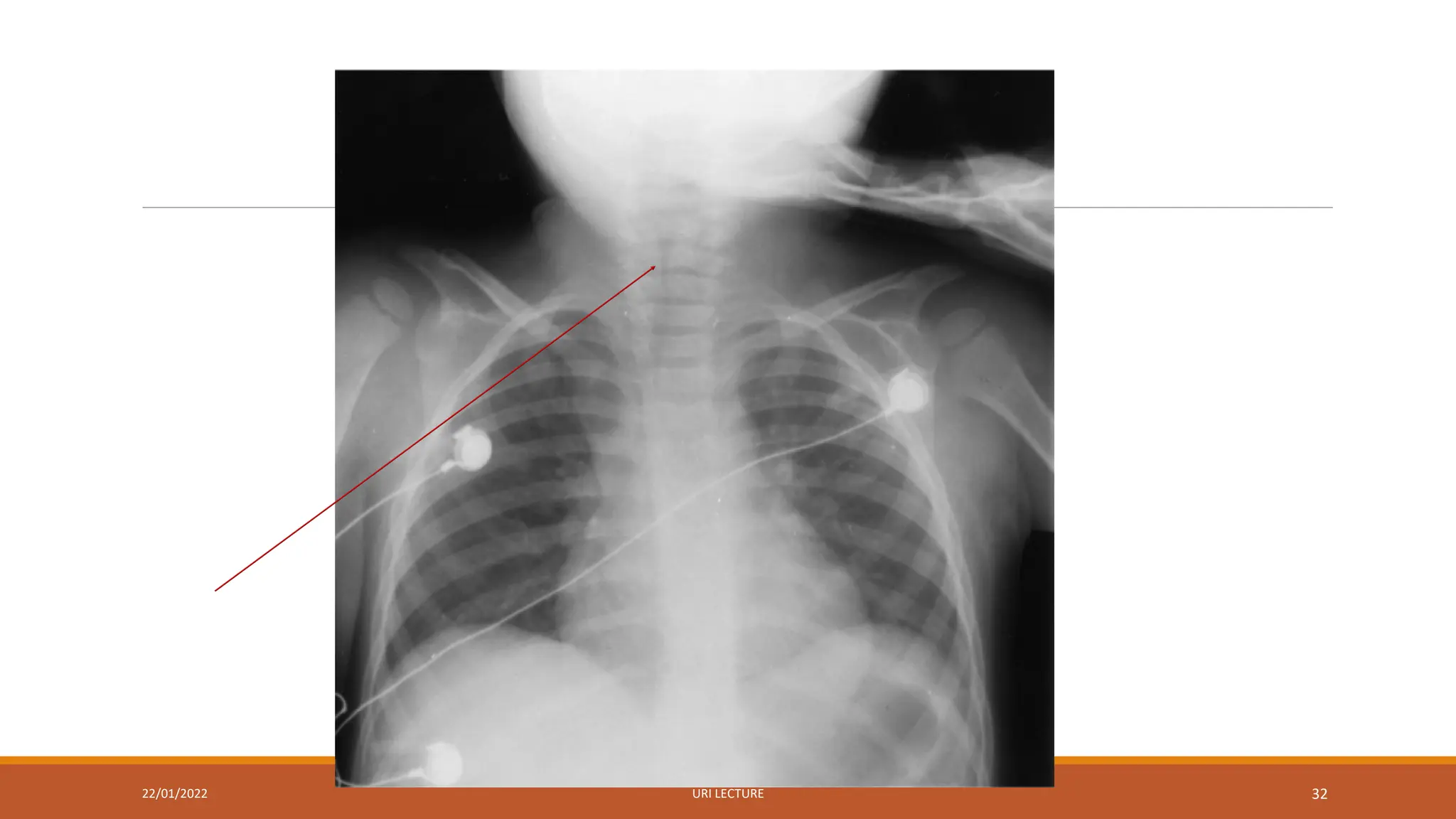
Diagnosis of LTB
Thediagnosis is clinical
X-rays may show the typical subglottic narrowing
22/01/2022 URI LECTURE 31
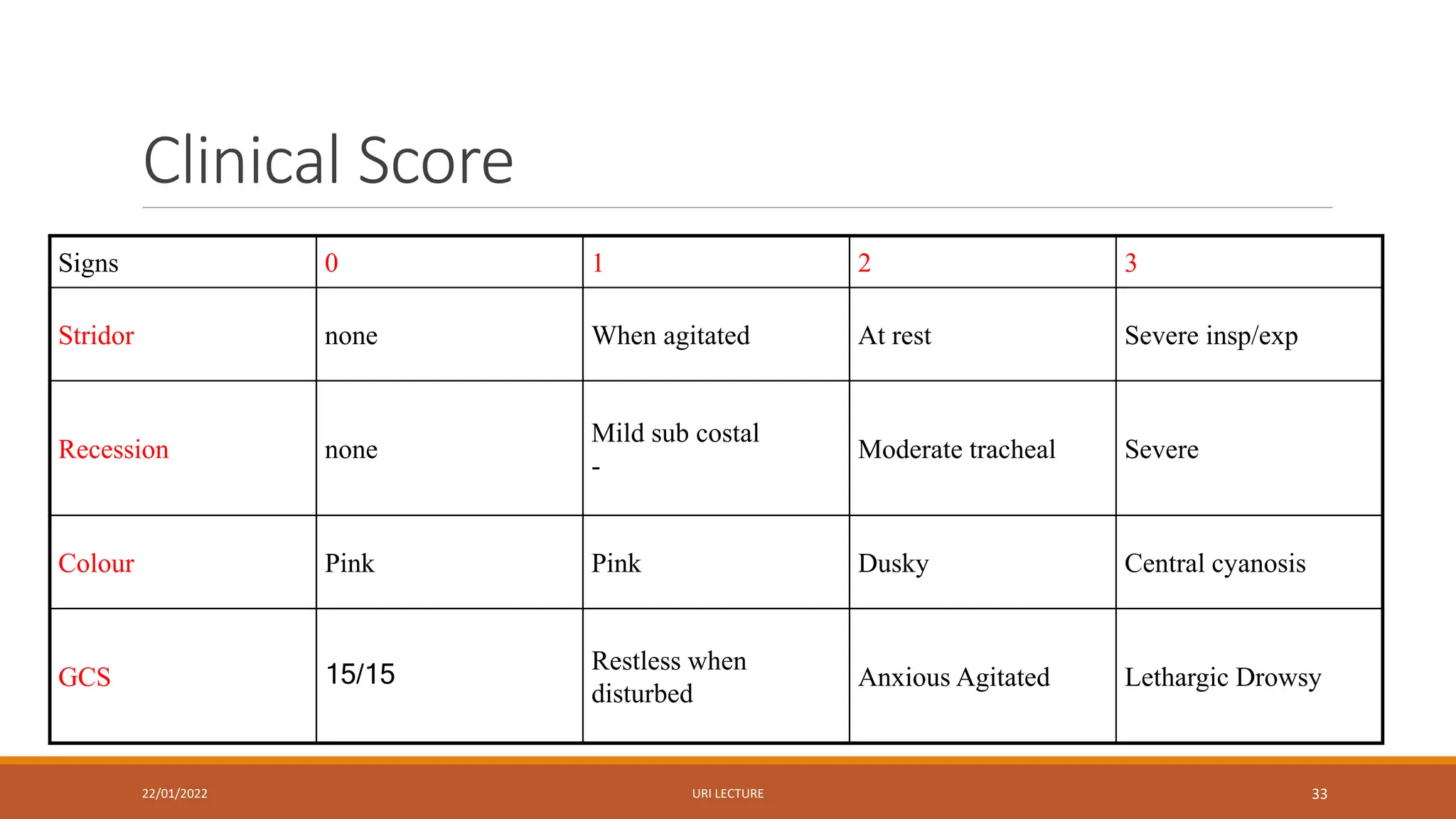
Clinical Score
22/01/2022 URILECTURE 33
Signs 0 1 2 3
Stridor none When agitated At rest Severe insp/exp
Recession none
Mild sub costal
-
Moderate tracheal Severe
Colour Pink Pink Dusky Central cyanosis
GCS 15/15
Restless when
disturbed
Anxious Agitated Lethargic Drowsy
34.
Score < 3Mild Croup
Can be allowed home
Advice to parents:
Increase oral fluids
Signs of increasing distress
Return to hospital or clinic
Easy access to the hospital
Consider oral dexamethasone 0.3mg/kg stat
22/01/2022 URI LECTURE 34
35.
Score 4-5 (moderatecroup)
Admit to the hospital
Oral dexamethasone 0.6mg/kg (max 4mg)
Budesonide Nebulization
1mg BD<1year
2mg BD>1year
22/01/2022 URI LECTURE 35
If score isstill ≥ 6
Repeat epinephrine neb
Call anaesthetist and ENT surgeon
Prepare for intubation
Consider tracheostomy
IV fluids
IV dexamethasone
Check ABG
If scoring < 6, follow moderate croup protocol
22/01/2022 URI LECTURE 37
38.
Case 4: Musonda
7-year-oldmale school age child
Coryzal symptoms for 2 weeks
Unable to smell
Has had dental pain for the last 4 days
Headache exacerbated by leaning forward
22/01/2022 URI LECTURE 38
39.
On examination
Temperature: 39.5oC
Purulent discharge from the right nostril
RR: 24 breaths per minute
HR: 110 breaths per minute
Localized pain over the cheekbones
22/01/2022 URI LECTURE 39
Sinusitis
It is acommon illness of childhood
It can be viral or bacterial
Bacteria include Streptococcus pneumoniae, nontypable Haemophilus influenza
and Moraxella catarrhalis
22/01/2022 URI LECTURE 43
44.
Clinical Manifestations ofSinusitis
Nasal congestion, purulent nasal discharge, fever and cough
Pain or pressure exacerbated by bending forward
The symptoms tend to localize the affected sinus in older children
22/01/2022 URI LECTURE 44
Diagnosis and treatmentof Sinusitis
The diagnosis of bacterial sinusitis is based solely on the history
According to the American Academy of Paediatrics, any URTI with any of the
following:
1. Persistent nasal discharge of any type or cough lasting 10 days or more without improvement
2. Worsening course (new or worse nasal discharge, cough or fever) after initial improvement
3. Severe onset, fever of 390 C and above for at least 3 consecutive days
22/01/2022 URI LECTURE 46
Complications of Sinusitis
Periorbitalcellulitis
Orbital cellulitis
Epidural abscess
Meningitis
Cavernous sinus thrombosis
Subdural empyema
Brain abscess
Osteomyelitis of the frontal bone
(Pott’s Puffy Tumour)
22/01/2022 URI LECTURE 48
49.
References
1. Nelson Textbookof Paediatrics 20th Edition
2. Rheumatic Fever-new diagnostic criteria. Izabela Szczygielska et al. Reumatologia 2018
3. Common Respiratory Infections Slides Dr Somwe wa somwe
22/01/2022 URI LECTURE 49