Acute Epiglottitis
Aetiologicagent is Haemophilus Influenza type B.
Strep pyogenes, Staph aureus, S. pneumonia are rarely
implicated
It is a life-threatening illness which runs a fulminant course within a
few hours if untreated
Occurs in children aged 2-7yrs with a peak age incidence of 3 yrs
Incidence rate is 6-14/ 100,000
3.
Symptoms
Sudden onset inyounger children or insidious over a
few hours from URTI in older children
Symptoms include:
-sore throat
-High grade fever
-Drooling of saliva
-Odynophagia or dysphagia
4.
Symptoms
-Muffled dysphoniaor aphonia
-Dry cough or no cough
-Difficulty breathing
-Constitutional upset- restlessness, irritability, fatigue,
-Alteration of consciousness
5.
Physical Findings
Position-classical tripod posture with a child sitting
upright supported by the fully extended hands with
head leaning forward and tongue hanging out.
Drooling of saliva
Respiratory distress- tachypnoea, dyspnoea
(suprasternal, supraclavicular ± intercostal, subcostal
or infrasternal)
6.
Physical Findings
Vitalsigns- Fever, Cyanosis, Small volume pulse
Pulse oximetry- Reduced oxygen saturation
Tender cervical lymphadenopathy
Tenderness over the larynx elicit by gentle palpitation
Stridor- inspiratory stridor heard maximally over anterior trachea. With
worsening obstruction, there may be disappearance of the stridor
7.
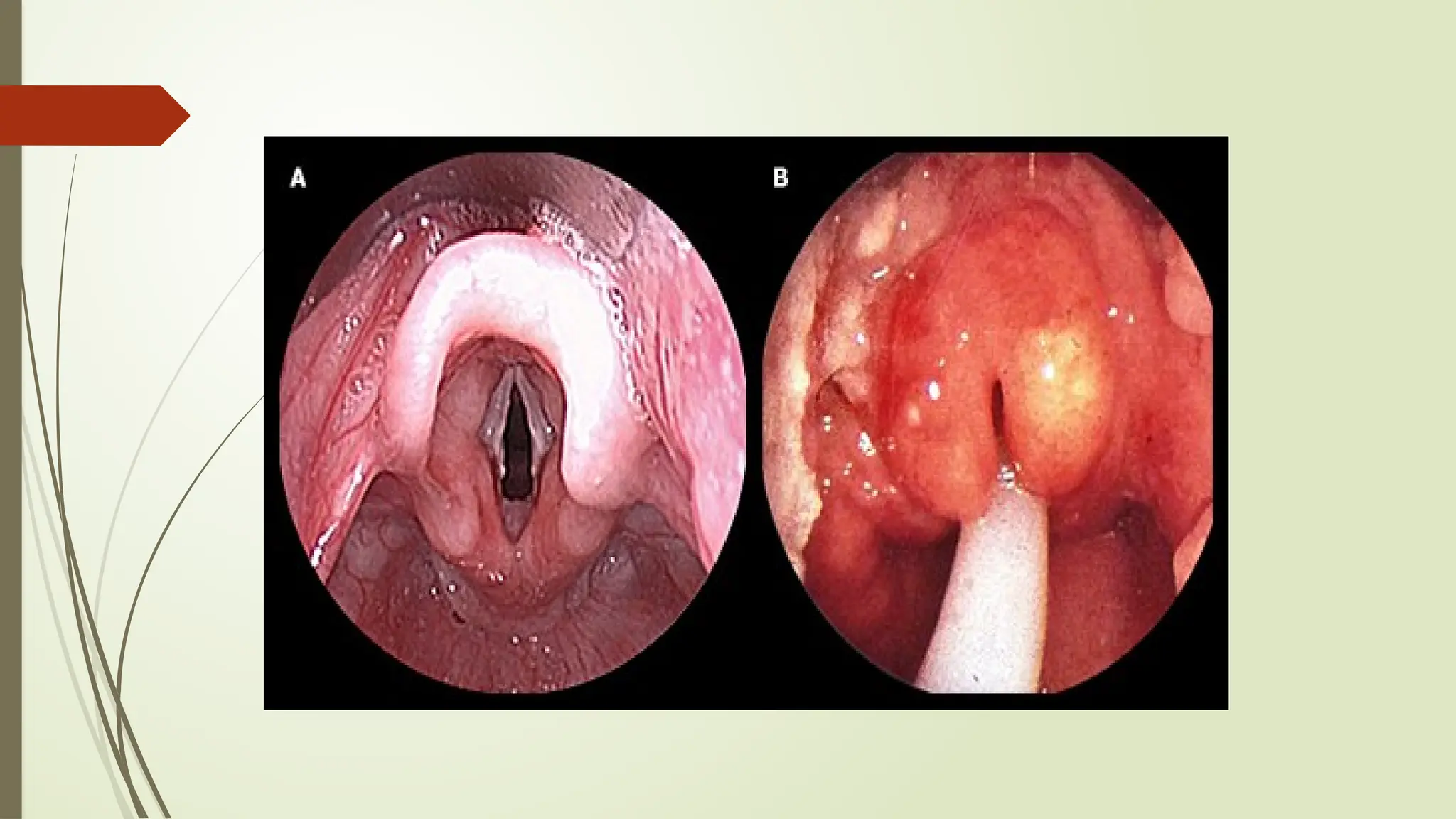
Physical Findings
Laryngoscopy-Gold standard for definitive diagnosis is direct oro-
pharyngeal visualization by using a tongue depressor and
laryngoscope.
However, this could provoke laryngospasm, compromise airway and
result in death.
Therefore, direct examination should only be done when Emergency
Endotracheal Intubation or Cricothyroidotomy can be safely
performed
Epiglottis appears as a swollen and cherry-red mass associated with
inflammation of surrounding structures.
9.
Laboratory Findings
Bloodculture- Positive for H. influenza in >80% of patients.
Chest X-Ray- Positive in only about 50% of patients.
-Use is limited in diagnosis.
-Inflammed epiglottis is seen as a shape of the thumb on
lateral neck X-ray.
Moreover, recumbent positioning could trigger respiratory
compromise.
11.
Laboratory Findings
CTscan – may be superior in delineating the soft tissue structure of
upper airway
-Usually unnecessary.
FBC- leucocytosis with neutrophil predominance
-Shift to the left
Oropharyngeal swab M/C/S- sample may be taken during
laryngoscopy but because of contamination with upper airway
flora, cultures may not be reliable.
Aspirate M/C/S of epiglottis abscess
12.
Treatment
Multi-disiplinary approach-Co-ordinated by the paediatricians but
supported by anaesthesiologist and ENT surgeons
Monitor vital signs and oxygen saturation to determine degree of
hypoxemia from respiratory fatigue, airway obstruction or laryngospasm
Oxygen if indicated– humidified. Dry oxygen worsens inflammation
Nil per oral
Hydration- To replace loss from resp distress, fever or drooling and for
calories due to odynophagia or dysphagia.
- Replacement is by IVF
13.
Treatment
Antibiotics- Empiricalbased on probable sensitivity- 2nd
generation Pencillins (β-lactamase) or 2nd
/3rd
gen
cephalosporins
Given Intravenously
Modify antibiotics with result of cultures
Glucocorticoids- to reduce inflammation. By IV or inhaled.
Of doubtful efficacy.
Avoid sedatives as they may suppress respiratory drive
Avoid instrumentation
Prevention- immunization against H. influenza B
Laryngotracheobronchitis (Croup)
A respiratoryinfection of the larynx and trachea but
may extend to the bronchi
Mainly caused by parainfluenza virus(80%) I>II & III
A common paediatric illness accounting for 15% of
clinic ± ER visits for ARI
Mostly a mild self-limiting illness
17.
Croup cont
Affectschildren aged 6m-6yrs with peak age in
second year
Usually single episode with only 5% of patients having
a second episode at >4-6 yrs
Majority of patients recover without sequlae but may
be life-threatening due to narrowing of larynx and
trachea below the glottis; Mortality Rate= <0.5%%
18.
Pathophysiology
Spread byinhalation of virus through nasopharynx and extension
of the infection to the larynx, trachea ± bronchi
Inflammation and oedema of the larynx and trachea at the
cricoid cartilage which is the narrowest part of the paediatric
airway
Areas involved have cellular infiltrates (lymphoctes, histiocytes,
plasma cells, neutrophils)
Activation of chloride secretion and sodium absorption across
tracheal epithelium contributing to oedema
19.
Pathophysiology
Epithelial damage andloss of ciliary function
Thick fibrinous exudate in the lumen of the trachea
These will result in significant reduction in airway
diameter causing partial airflow obstruction
Oedema of vocal cords causes reduced mobility
resulting in hoarseness
20.
Symptoms
Clinically twovarieties:
-Infectious croup: viral cause
-Spasmodic croup: viral modified by allergic response
Infectious Croup
Insidious onset
Preceeded by URTI with symptoms worsening at night such
that most ER visits are between 10pm-4am
Fever: low grade or absent
Characteristic barking cough- typical cough evolves over
days
21.
Symptoms
Inspiratory stridor- progressesfrom with agitation to
even at rest
Hoarseness
Respiratory distress- depends on degree and extent
of obstruction;
nasal flaring
suprasternal
intercostal recessions
Symptoms resolve within 3-7 days but may last for 2
weeks
22.
Symptoms
Spasmodic croup
Suddenonset of barking cough, Stridor and Resp distress
In an otherwise well child except for very mild URT symptoms
Does not have an insidious progression of Stridor and Cough
23.
Physical Findings
Variable dependson degree of
obstruction
Not toxic looking- may be restless, agitated
Respiratory distress variable- Dyspnoea: nasal
flaring, recessions
Pulse oximetry- Hypoxia depends on degree of
obstruction
24.
Physical Findings
• InspiratoryStridor with exertion. In progressive severity,
stridor is present in expiration, at rest or absent
• Rhonchi with bronchial involvement
• Other findings in severe cases:
• Lethargy
• inability to drink
• Tachypnoea
• Tachycardia more than due to fever
• Hypotonia
• Cyanosis
25.
Physical Findings
Clinicalscoring (westley)- To assess the degree of respiratory
compromise using 5 criteria
-Inspiratory Stridor
None=0, on agitation=1, at rest=2
-Retractions
Mild=1, moderate=2, severe=3
-Air entry
Normal=0, mild decrease=1, marked decrease=2
26.
Clinical Features
-Cyanosis
None=0, onagitation=4, at rest=5
-Level of consciousness
Normal=0, altered/ depressed=5
Summary
Mild disease= <3
Moderate disease= 3-6
Severe disease= >6
27.
Diagnosis
Mainly clinical.Laboratory studies- rarely contributory:
1) FBC- Lymphocytosis of viral infections
2)Imaging studies- Chest radiograph reveals the
classical ‘steeple’ sign due to subglottic narrowing.
3)Laryngoscopy- Unnecessary except in unusual
presentations or possible superinfection.
4) Tracheal aspirate M/C/S- for possible bacterial
superinfection
29.
Treatment
Depends ondegree of airflow obstruction
Majority are mild and only parental reassurance and education are
required. Managed as an out-patient
Moderate to severe cases should be admitted
Ensure comfort, avoid agitations as these worsen obstruction,
respiratory fatigue and increases oxygen need
Close monitoring of vital signs and oxygen saturation to assess
deterioration
30.
Treatment
A andB evaluation in ED.
Respiratory support
In moderate cases, give Supplemental Oxygen by nasal prong or
catheter
in severe compromise- give Oxygen by bag & mask or endotracheal
intubation
If an endotracheal intubation is indicated, the ET tube should be <0.5-
1mm less than predicted
Cool mist- moistens airway, reduces viscosity of secretions and soothes
inflammed mucosa
31.
Treatment
Corticosteroids- Anti-inflammatoryeffect.
- Standard treatment protocol in mild-moderate cases as it
reduces laryngeal mucosal oedema.
- Single dose dexamethasone 0.6mg/kg IV/IM/PO should be given
within 24hrs of illness
Nebulized racemic L-epinephrine.
-Used in moderate to severe cases.
-Acts by adrenergic stimulation causing arteriolar constriction,
lower hydrostatic pressure and interstitial fluid resorption and
reduction in laryngeal oedema.
-Also, bronchial Ms relaxation and bronchodilatation
32.
Upper Respiratory TractInfections
Clinical
Diagnosis
Aetiological Agent Clinical Features Management
Rhinitis Rhinovirus,
coronavirus
rarely adenovirus,
influenza virus
Nasal congestion, rhinorrhea, mouth
breathing sneezing, conjuctivitis
Diagnosis – clinical
Treatment- supportive
Naso-pharyngitis Rhinovirus,
adenovirus,
enterovirus,
parainfluenza virus
Rhinitis with pharyngeal symptoms
(scratchy/ sore throat, dysphagia,
odynophagia) ± laryngeal and
constitutional symptoms
Diagnosis- clinical
Treatment- supportive
Acute
Pharyngitis
Viral- adenovirus,
enterovirus
Bacterial- Grp A
streptococcus,
diphtheria
Pharyngeal erythema, pharyngeal
exudate, tonsillar enlargement,
mucosal vesicles or erosions
Diagnosis- FBC, M/C/S or vi
cultures using pharyngea
swabs and Rapid Tests
Treatment: viral- supportive
bacterial- antibiotics
Acute Epiglotittis Haemophilus
influenza type b
Fever, sore throat, dysphagia, drooling,
dysphonia, dyspnea, dry cough, stridor,
in tripod position and later alteration of
consciousness. Fulminant course
Direct Laryngoscopy- cher
red swollen epiglottis, bloo
culture and rarely neck x-ra
Treatment- antibiotics
immunization
33.
Upper Respiratory TractInfections
Respiratory Infection Aetiologic Agent Clinical Features Management
Acute laryngo-
tracheobronchitis
(Croup)
Parainfluenza virus I; II or 111 Preceeded by URTI with symptoms
worsening at nights
Barking cough, inspiratory stridor,
horseness, progressive dyspnea and
minimal fever
Diagnosis- clinical.
Investigations rarely
helpful: steeple sign o
CXR, Lymphocytosi
Treatment: self-limiting
just re-assurance
In severe, supplemen
oxygen, cool mist an
corticosteroids ±
nebulized racemic
epinephrine
Otitis Media Strept pneumonia
Haemophilus influenza
Viruses-RSV, influenza
From nasopharyngitis
Fever, irritability, ear pain, loss of light
reflex with bulging tympanic
membrane, ear discharge at later
stage
Diagnosis: clinical b
supportive ear swab
M/C/S with ear discha
Treatment: Antibiotic
34.
Differences between Croupand Epiglottitis
Characteristics :
Epidemiology
Croup Epiglottitis
Prevalence Very Common Very Rare
Seasonality During warmer seasons- autumn,
summer
All throughout the year
Timing of Day Usually at nights Throughout the day, may worsen
at nights
Sex Predilection Males > Females Males = Females
Age Prevalence 6 months – 3 years 3 years – 7 years
35.
Characteristics: Pathology CroupEpiglottitis
Aetiology Viral Bacterial
Pathogenic Agent Para- Influenza virus I, II,III
RSV
Haemophilus Influenza type b
Pathology Significant Subglottic Inflx
Mucosal inflammation with
secretions
Oedema to level of Larynx
Significant Supralottic inflx
Inlammation and oedema at level
of Epiglottis
Characteristics: Clinical Features
Preceeding URT Prodrome Yes, Usually No
Onset Insidious within 12-48 hours Abrupt/ sudden, within 2-4 hours
Appearance Well looking Toxic, acutely ill-looking
36.
Characteristics: Clinical FeaturesCroup Epiglottitis
Fever Moderate, < 38.5C High, > 38.5C
Cough Barking, seal-like quality Minimal, may be absent
Stridor Loud Inspiratory, may be biphasic
Mild to moderate
Soft Inspiratory
Moderate to Severe
Dyspnoea Variable Significant
Speech/ Cry Hoarse Soft, Muffled, Unable to speak
Dysphagia Able to swallow Drooling of saliva, Unable to
swallow
Posture Calm, Supine, Unremarkable Restless, Tripod Position
Sitting forward with neck
extended
37.
Characteristics: Investigations CroupEpiglottitis
White Blood Cells Normal Elevated
Laryngoscopy: site Involved Sub-glottic Supra-glottic
Radiology AP/PA view: Steeple sign
(TrAcheal Narrowing)
Lateral view: Thumb sign
( Swollen Epiglottis)
Characteristics: Treatment
Oxygen Therapy Humidified air, Oxygen only
if hypoxaemic -severe
Intubation and ventilation may be required
Drug therapy Racemic Epinephrine, IV/ IM
Dexamehasone or oral
Prednisolone
IV Antibiotics
38.
Other Causes ofStridor
• Bacterial Tracheitis
• Retro-pharyngeal Abscess
• Peri-tonsillar Abscess
• Foreign Body Aspiration in Trachea, Larynx
Lower Respiratory TractInfections
Respiratory Infections Aetiological Agents Clinical Features Management
Acute Tracheitis Staphylococcal
aureus
Rare and course is
insidious
Fever, toxic appearance,
inspiratory stridor, barking
cough, hoarseness but
no dysphagia
Diagnosis: clinical
CXR- Steeple sign,
sputum M/C/S
Treatment: IV antibiotics
No or limited response to
adrenaline
Bronchiolitis RSV, Influenza,
parainfluenza
Usually mild with insidious
course. URTI with persistent
cough, progressive
breathlessness, wheeze or
apnoea, irritability with
reduced feeding.
Tachypnoea, dyspnoea,
cyanosis, hyper-resonance,
prolonged expiration,
expiratory rhonchi with
palpable liver and spleen
Diagnosis: clinical.SP02 Blood
gas to determine degree of
obstruction. CXR, FBC, Viral
studies not helpful
Treatment: Supportive-
A,B,C,D
Bronchodilators and steroids
of doubtful efficacy
Ribavirin in severe cases
P N E U M O N I A
42.
Bacterial Tracheitis
Epidemiology
•Prevalence: Rare
• Age Prevalence: 3years – 10 years
• Pathogenic Agent; Staphylococcal aureus
Clinical Characteristics
• Onset: Insidious over 2-3 days, worsens within 10 hours
• Appearance: well to toxic
• Fever: Moderate to High grade
• Stridor: Mild Inspiratory Stridor
43.
Bacterial Tracheitis cont
•Cough: Barking quality
• Speech/ Voice: Hoarse
• Secretions: Mild secretions, No Dysphagia (able to swallow)
• Radiology: AP/PA view- Steeple sign (Shaggy Tracheal air
column)
• : Lateral view- Hazy
• Treatment: IV Antibiotics
• : Partial or No Response to Adrenaline