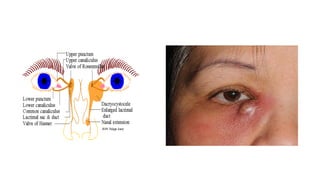
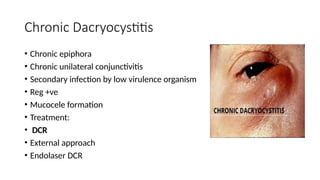
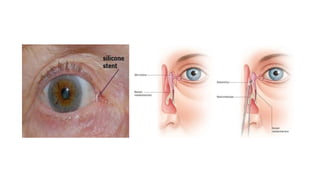
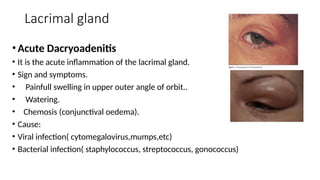
The document discusses various disorders of the lacrimal system, particularly obstruction of the nasolacrimal duct (NLD) leading to symptoms like tearing, discharge, and pain. It outlines causes, clinical presentations, and treatments for conditions such as dacryocystitis, acute dacryoadenitis, and keratoconjunctivitis sicca. Epidemiologically, women are more affected than men, and treatment options vary from medications to surgical interventions.