Downloaded 519 times
![Address: Oleg Kshivets, M.D., Ph.D. Consultant Thoracic/Abdominal Surgeon Department of Surgery Siauliai Public Hospital Tilzes:42-16, LT78206, Siauliai, Lithuania tel (37041)416614 e-mail: [email_address]](https://image.slidesharecdn.com/kshivetsneworleans1999-100810005916-phpapp01/75/Kshivets-O-Lung-Cancer-Surgery-31-2048.jpg)

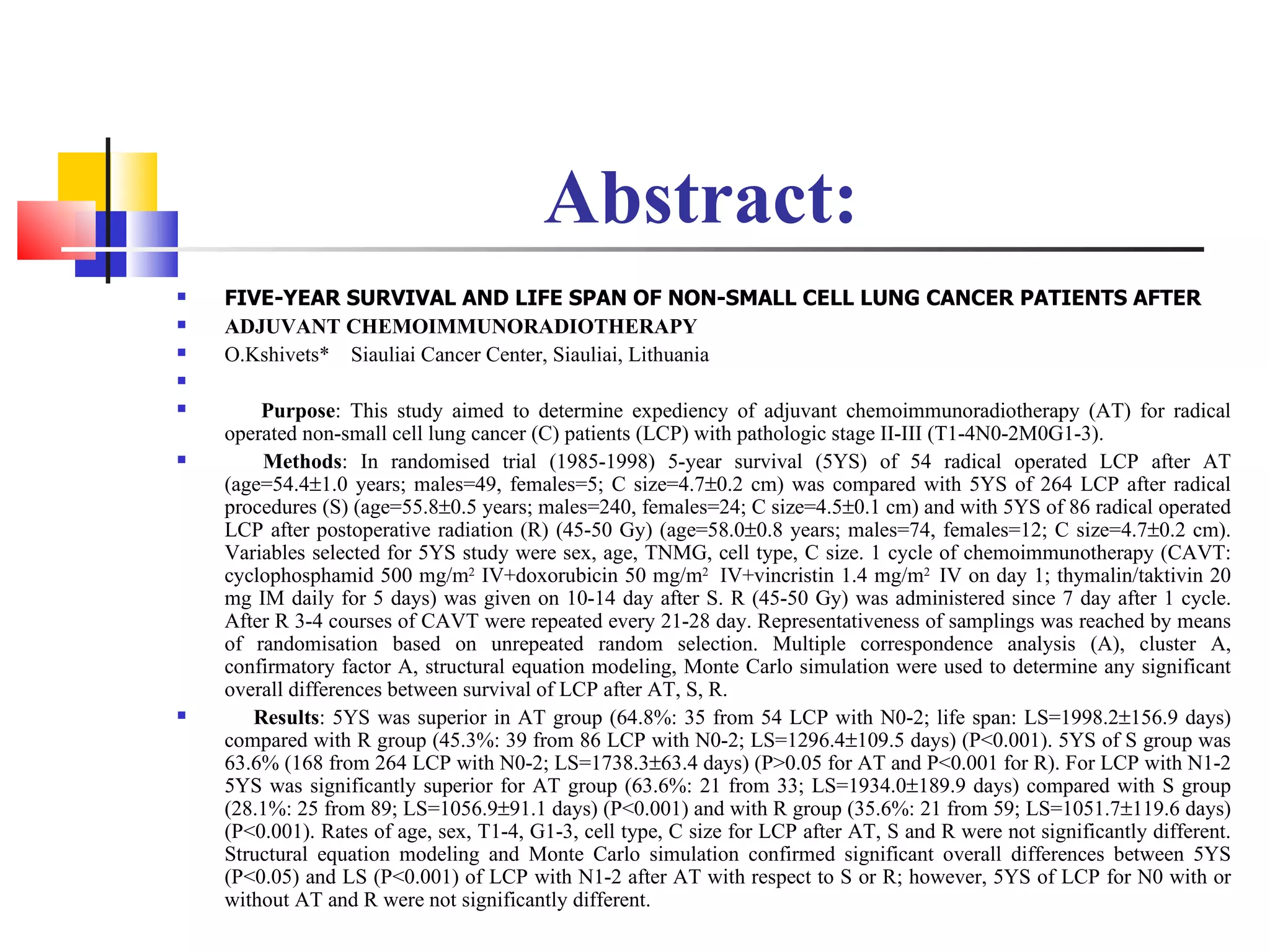
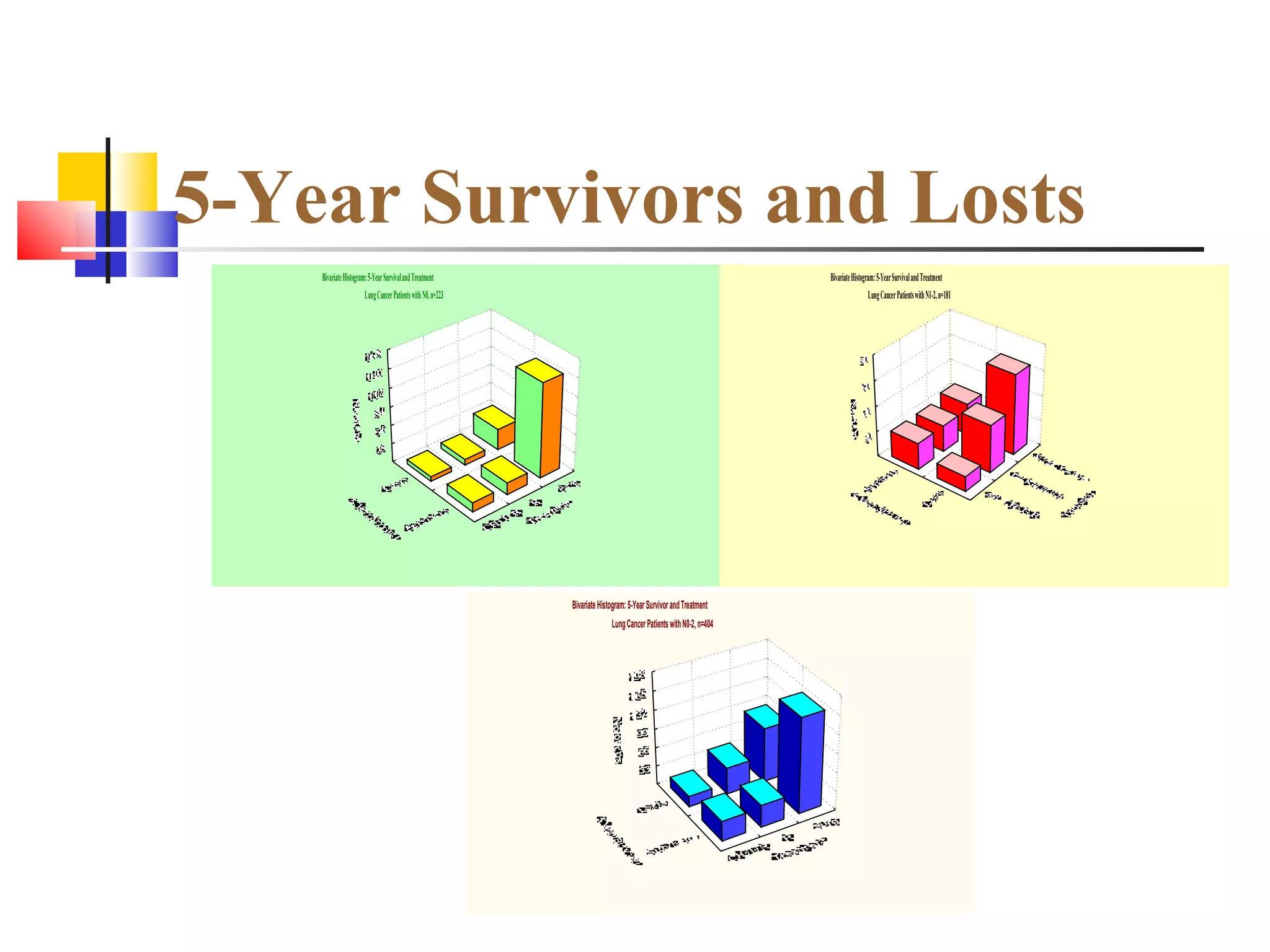
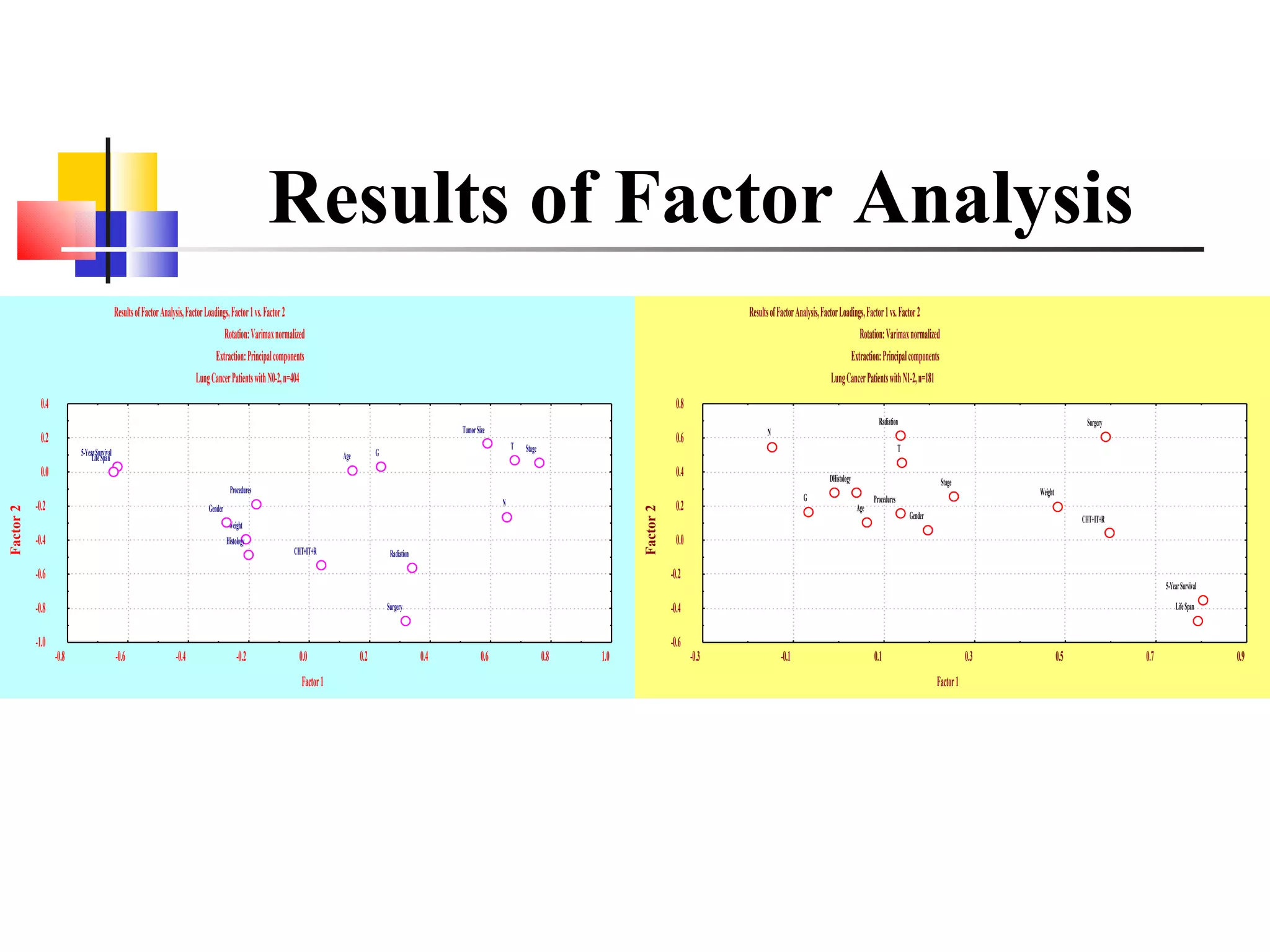
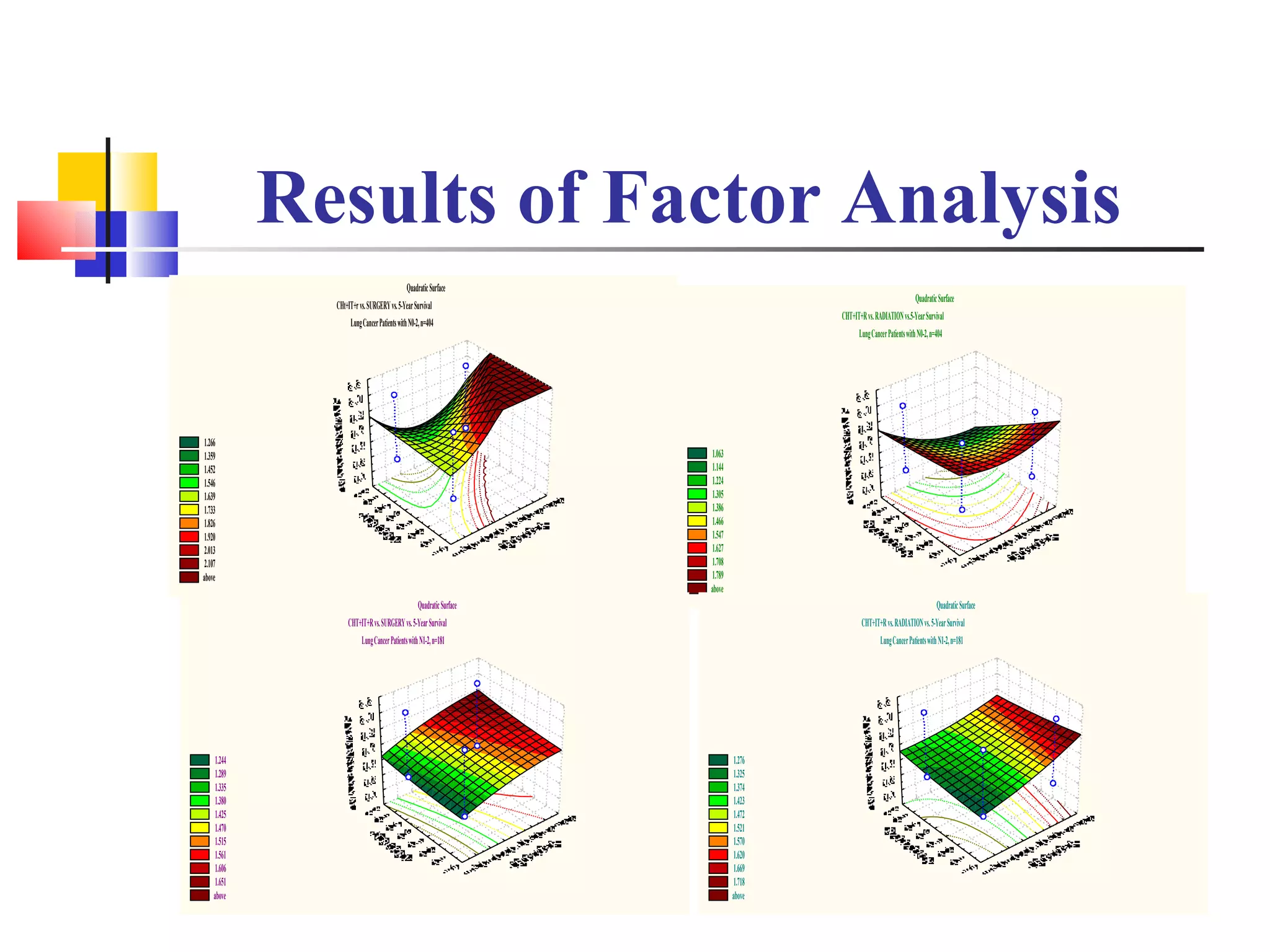
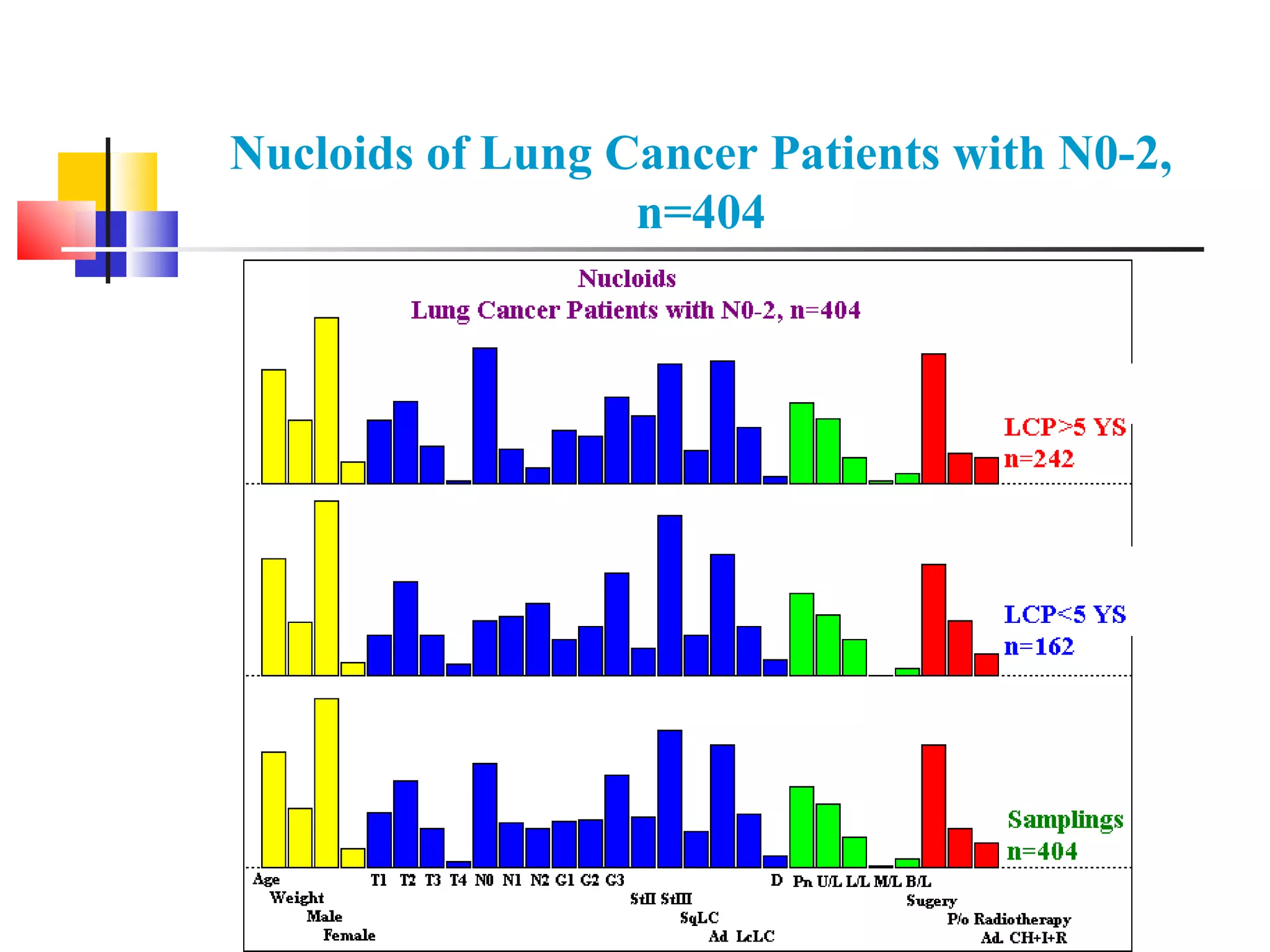
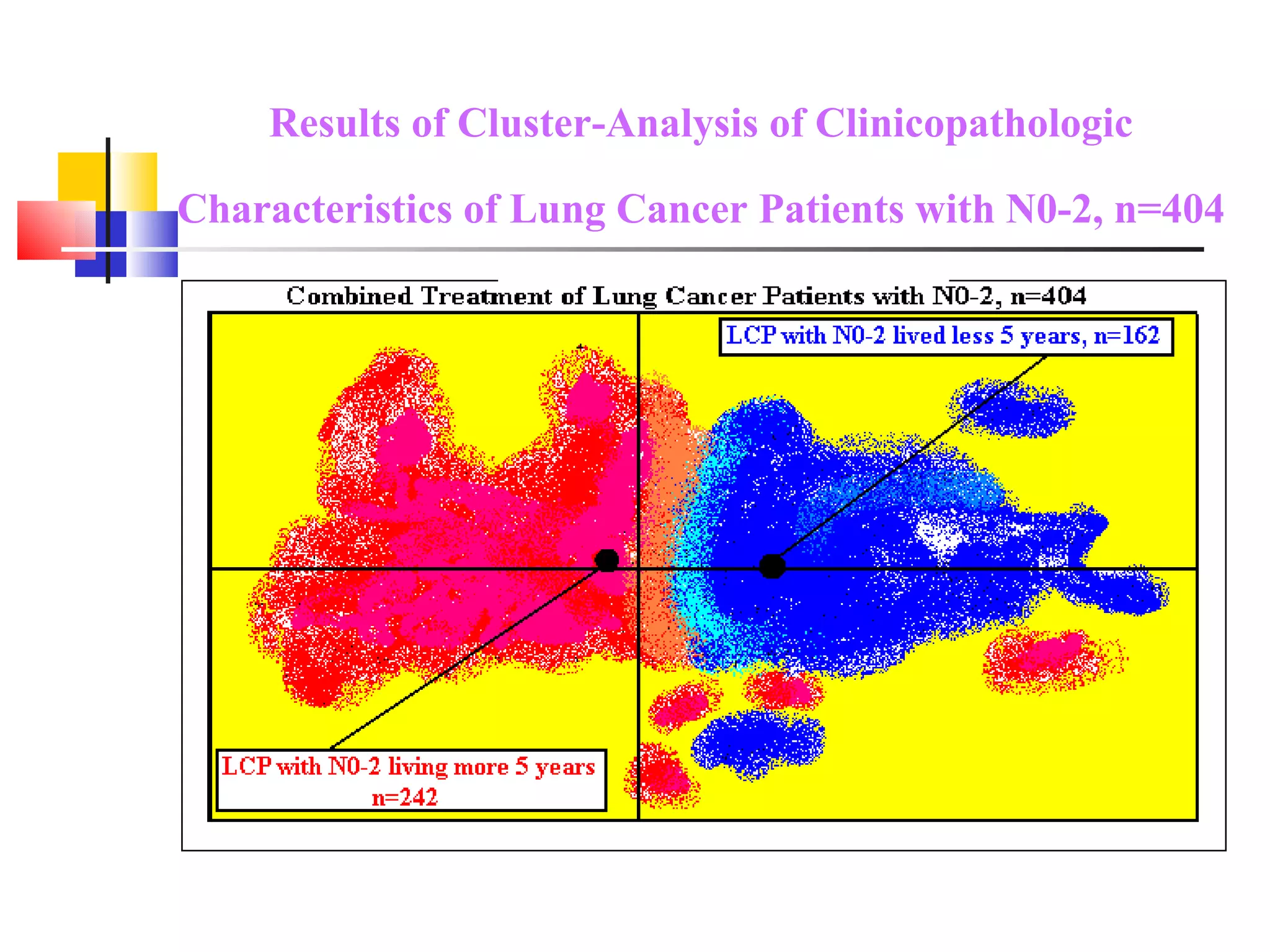
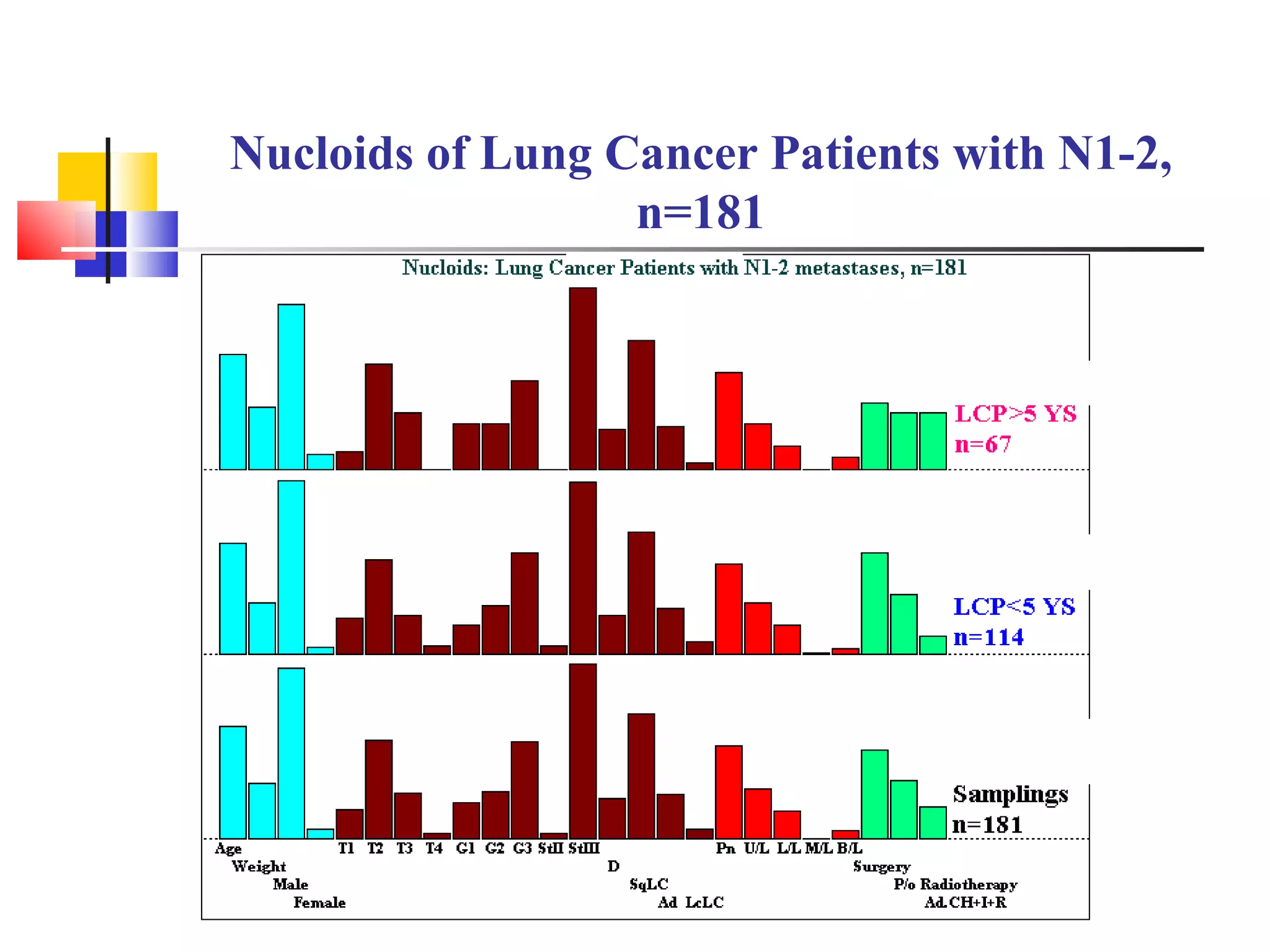
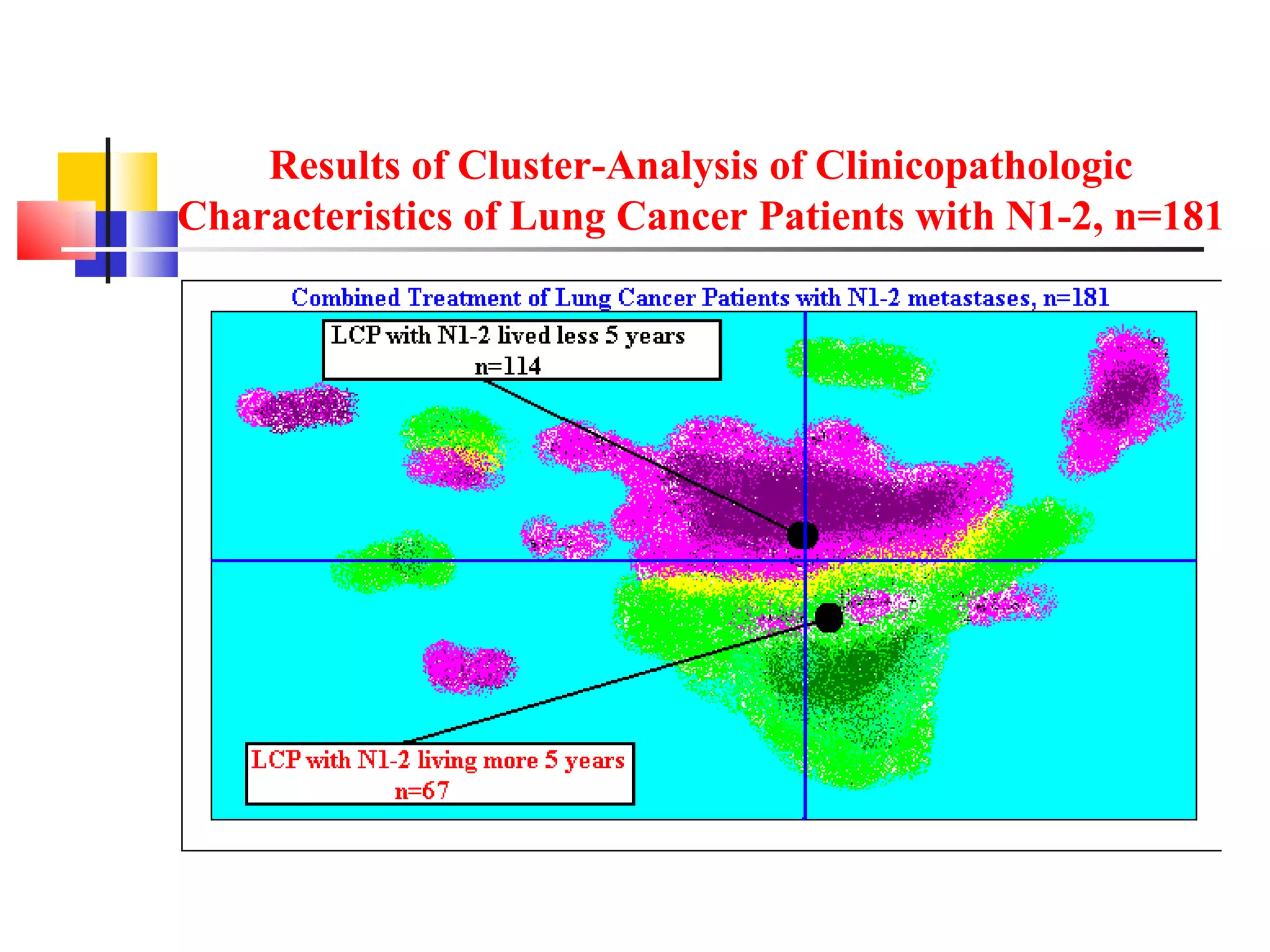
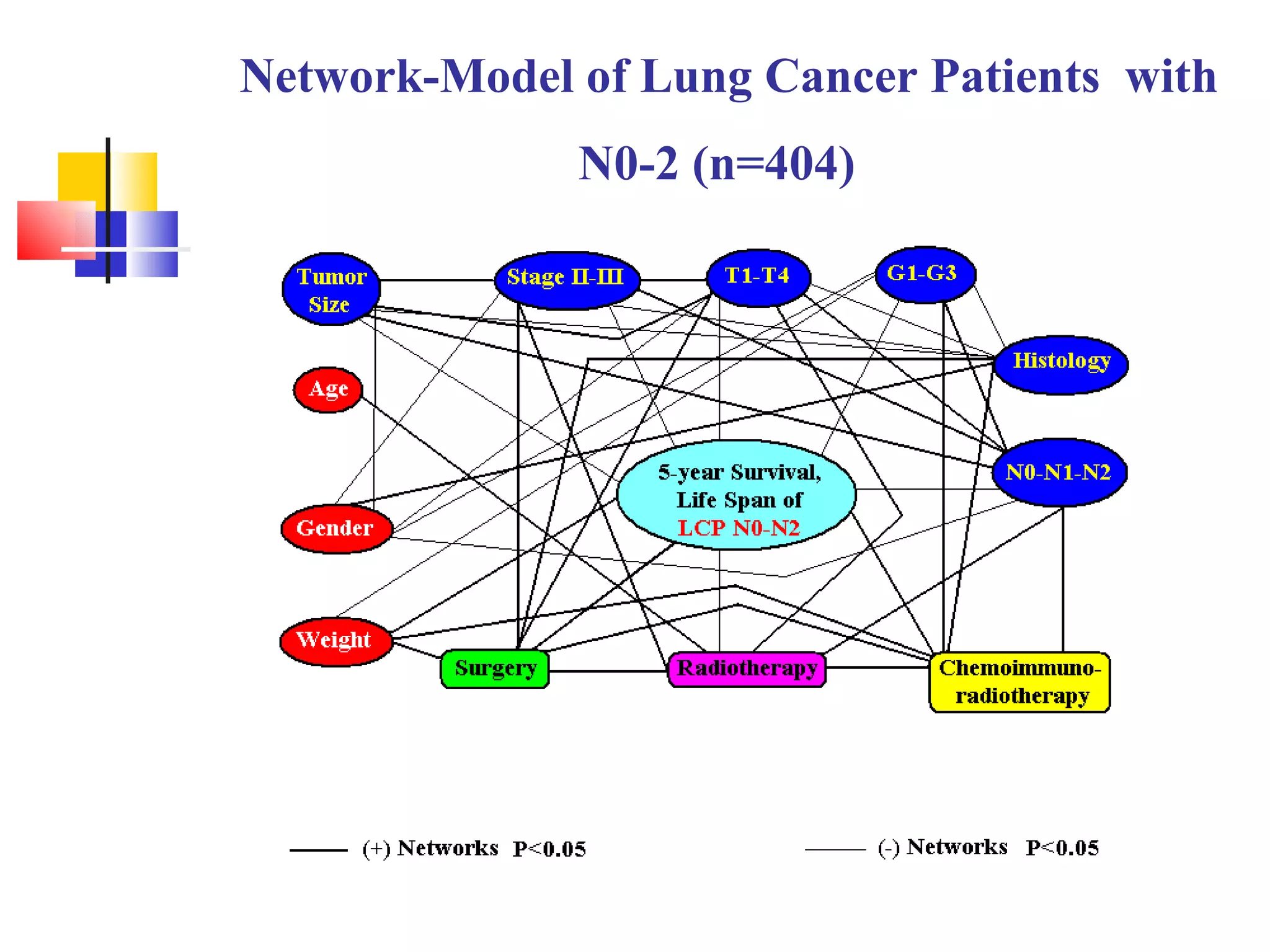
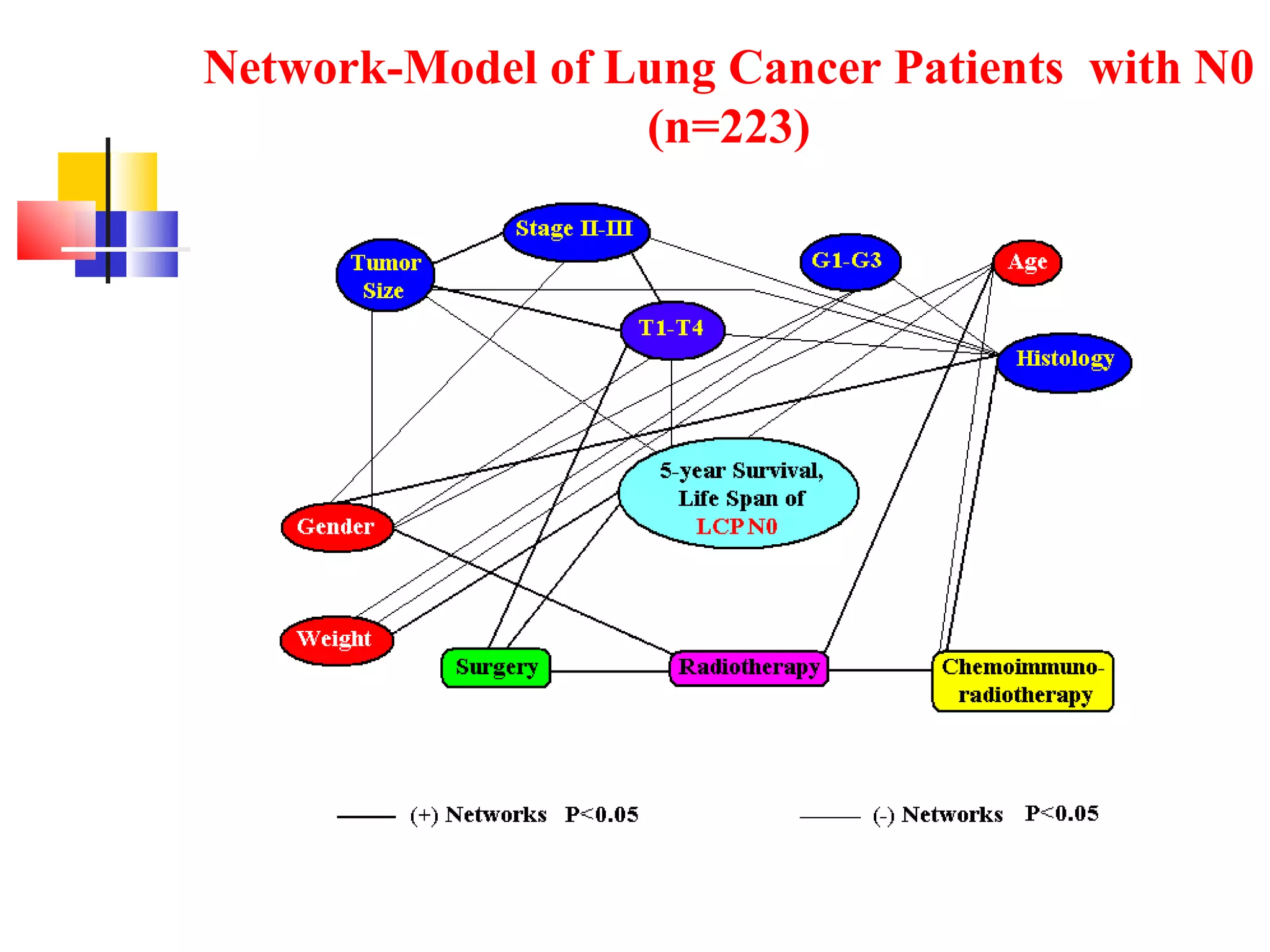
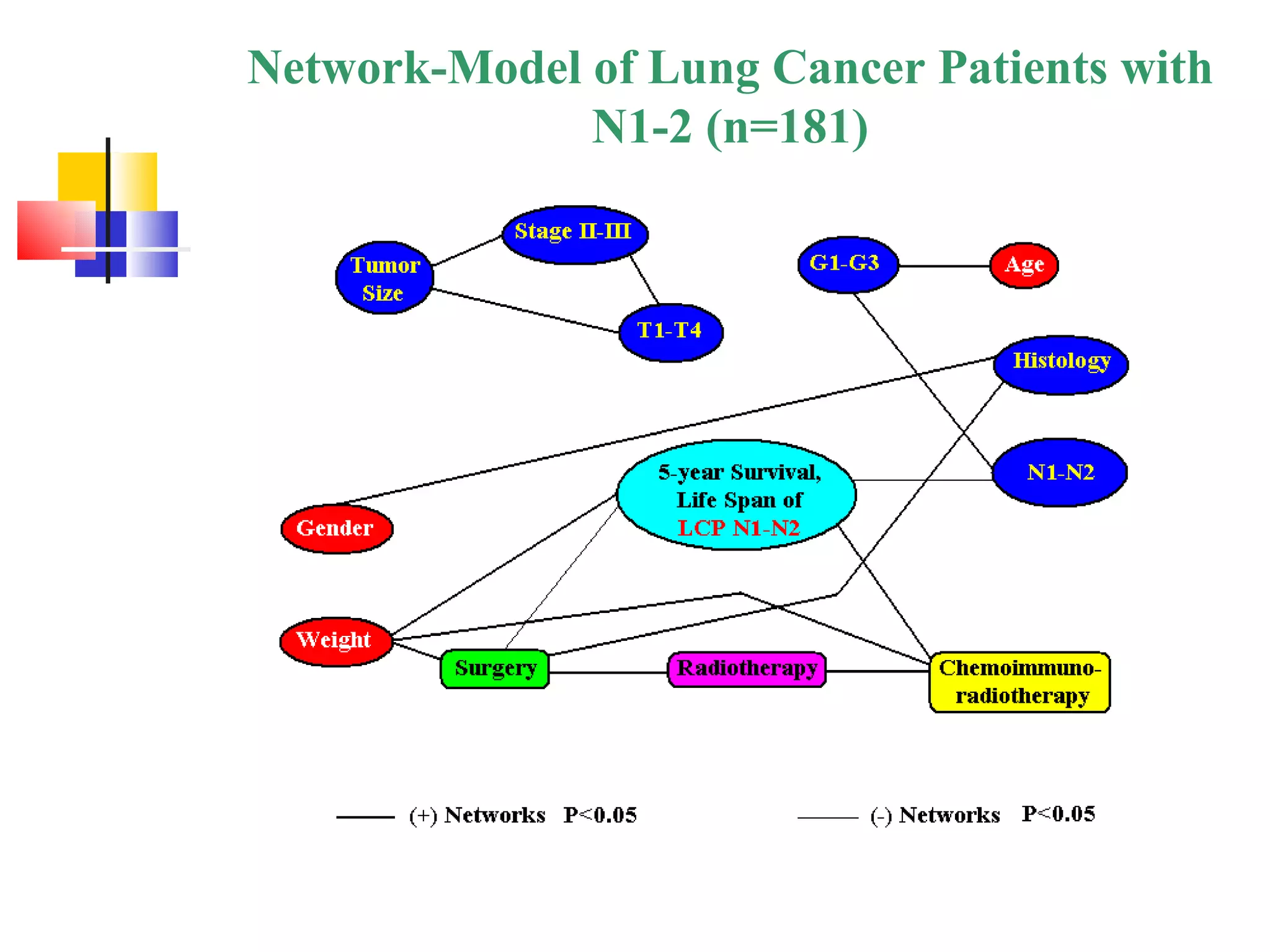
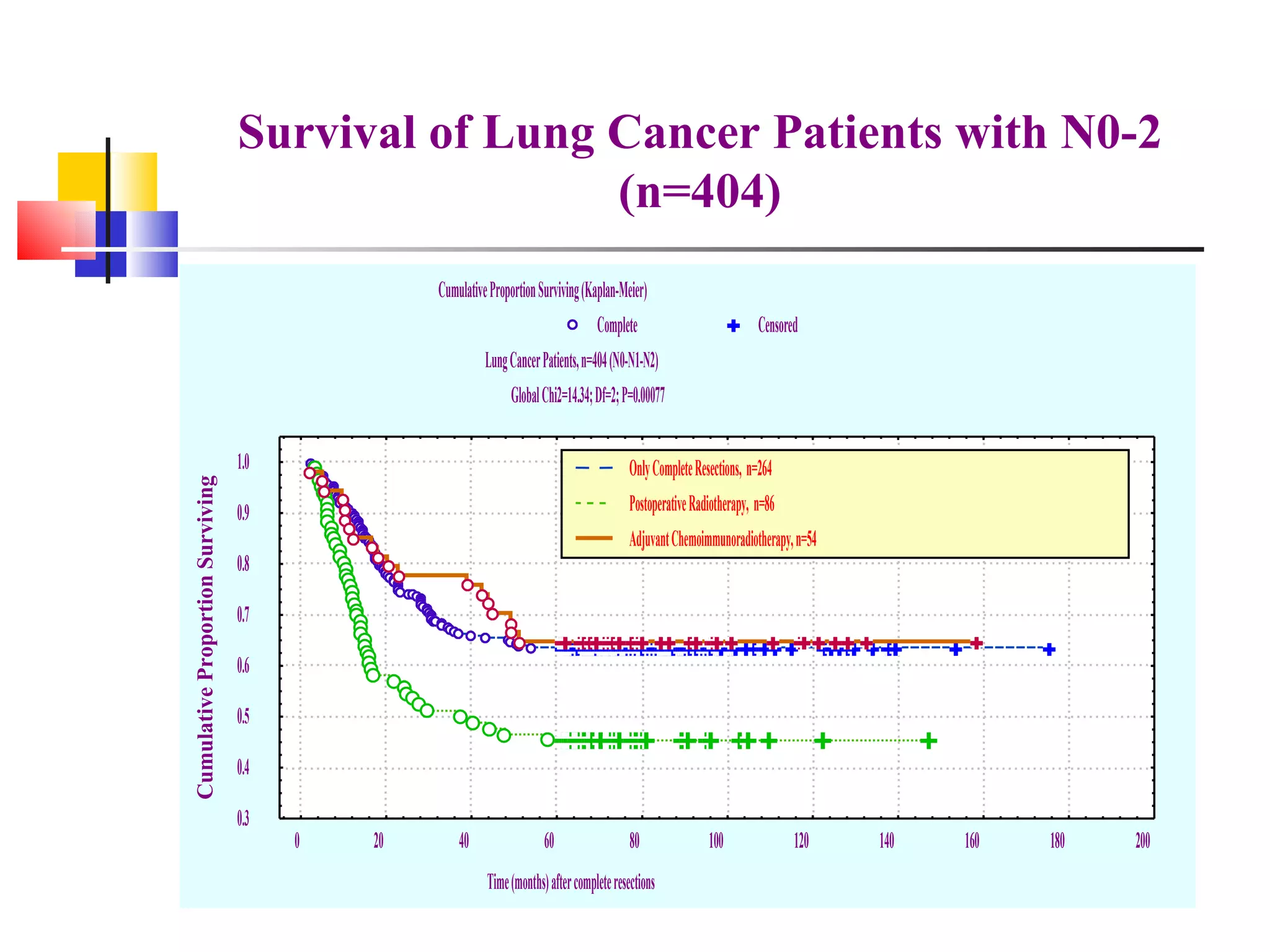
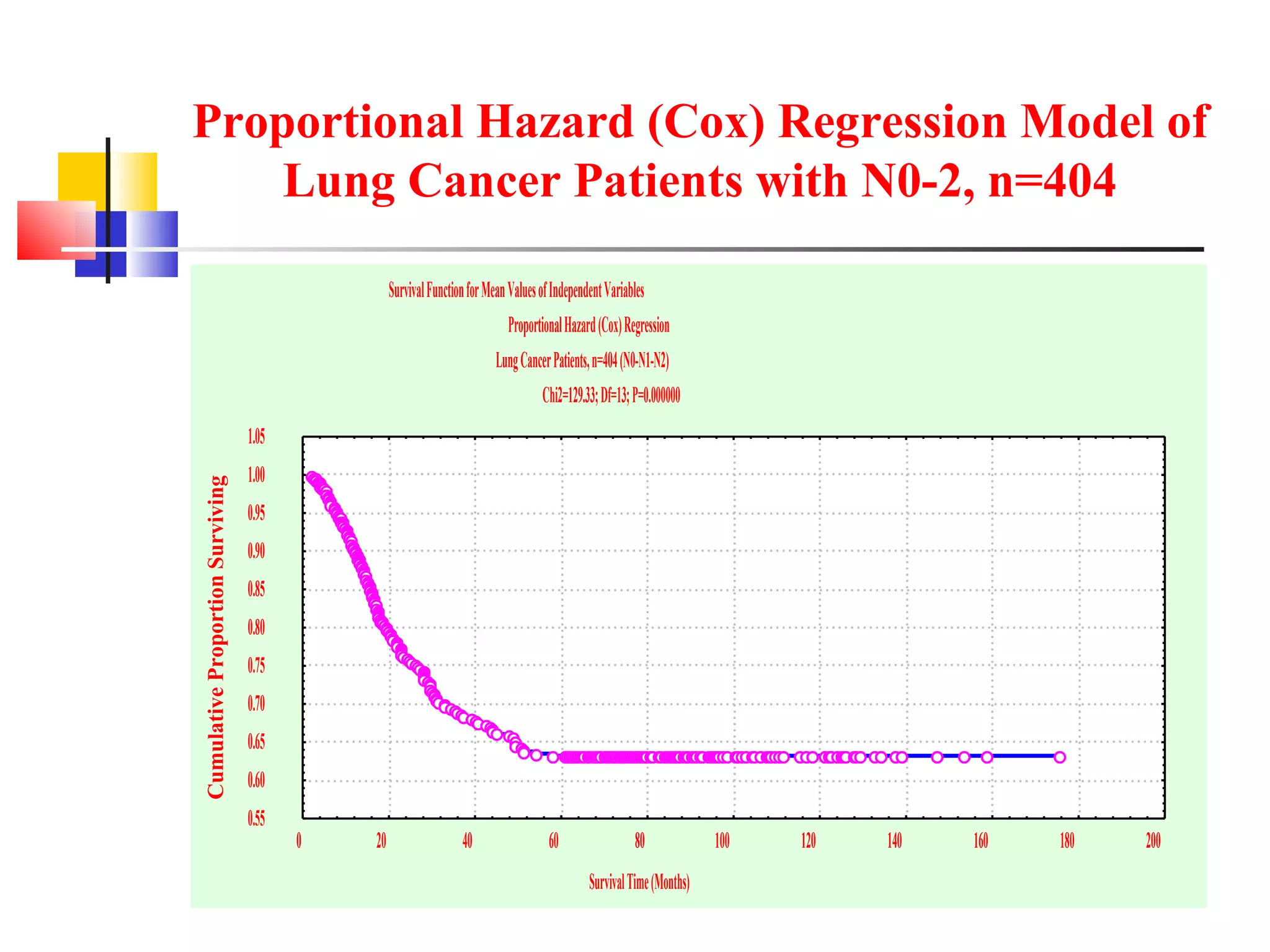
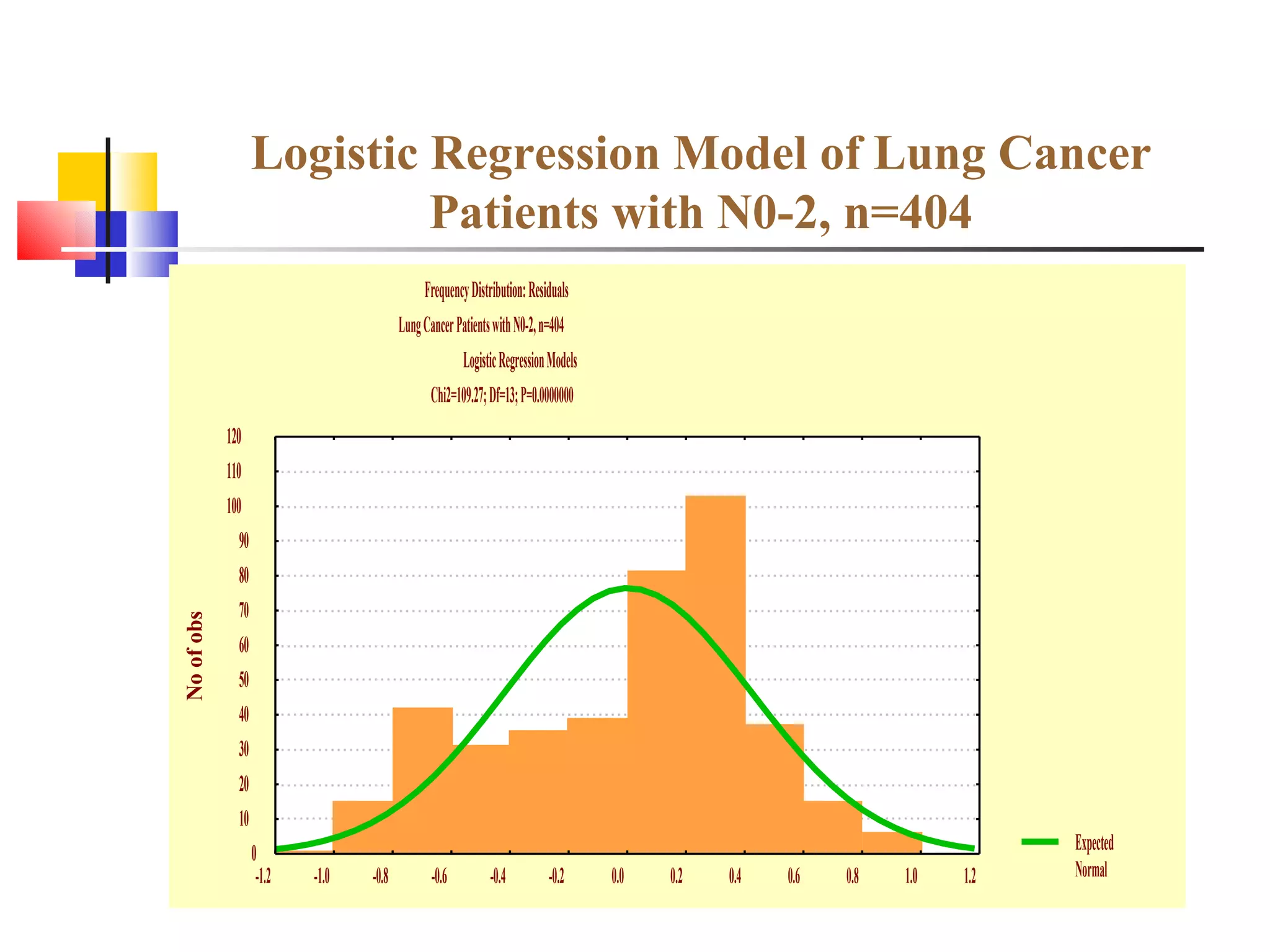
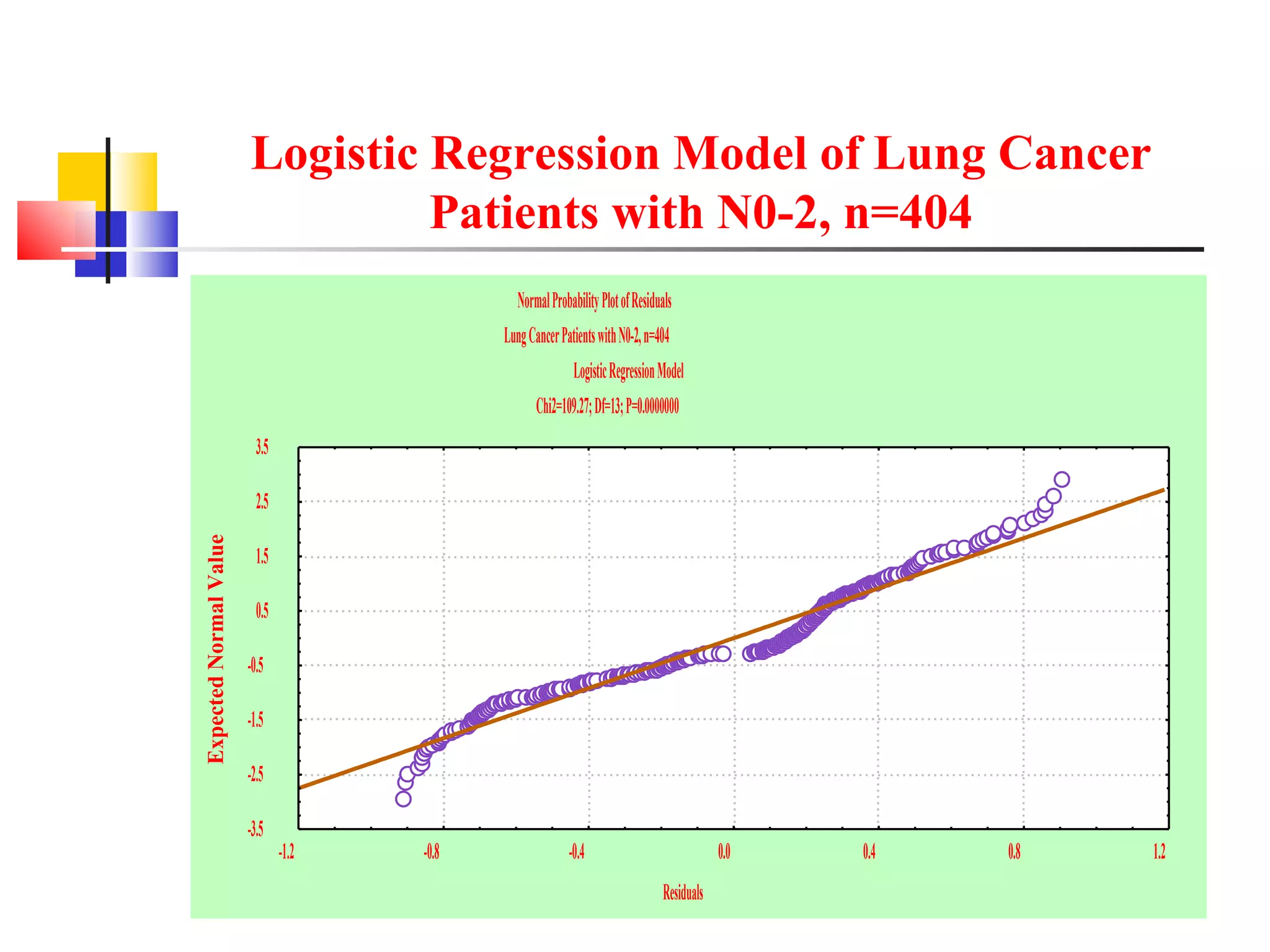
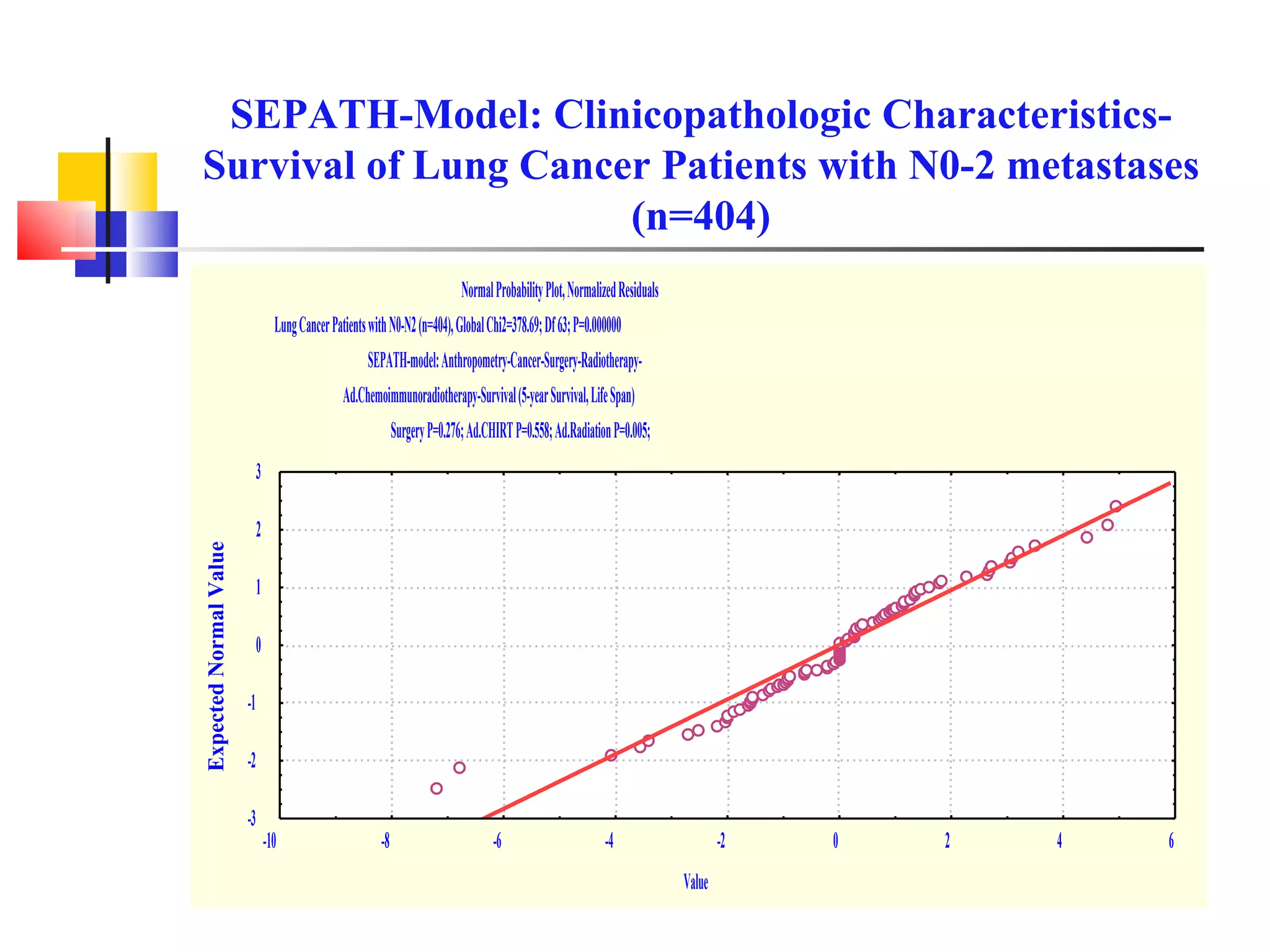
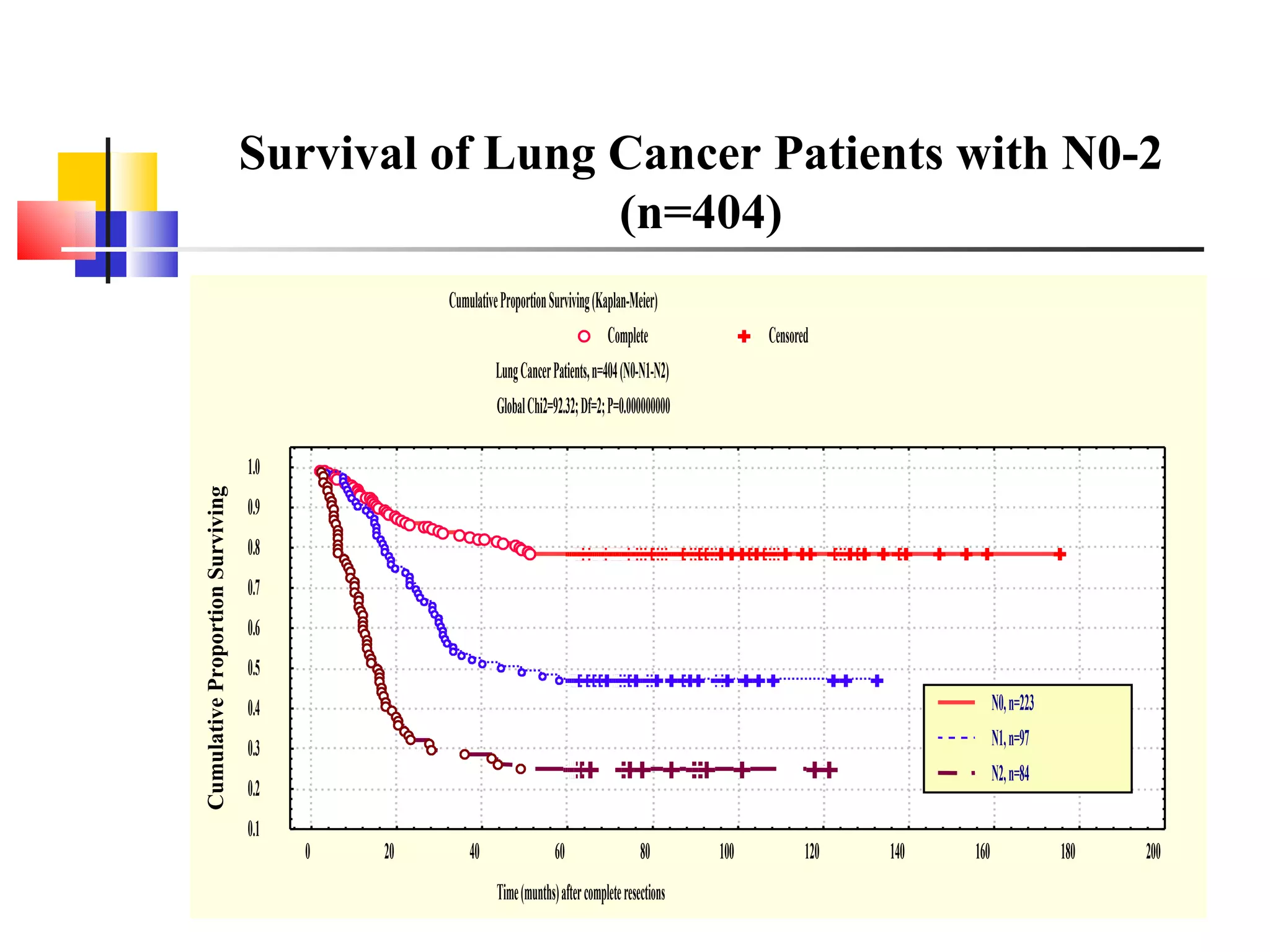
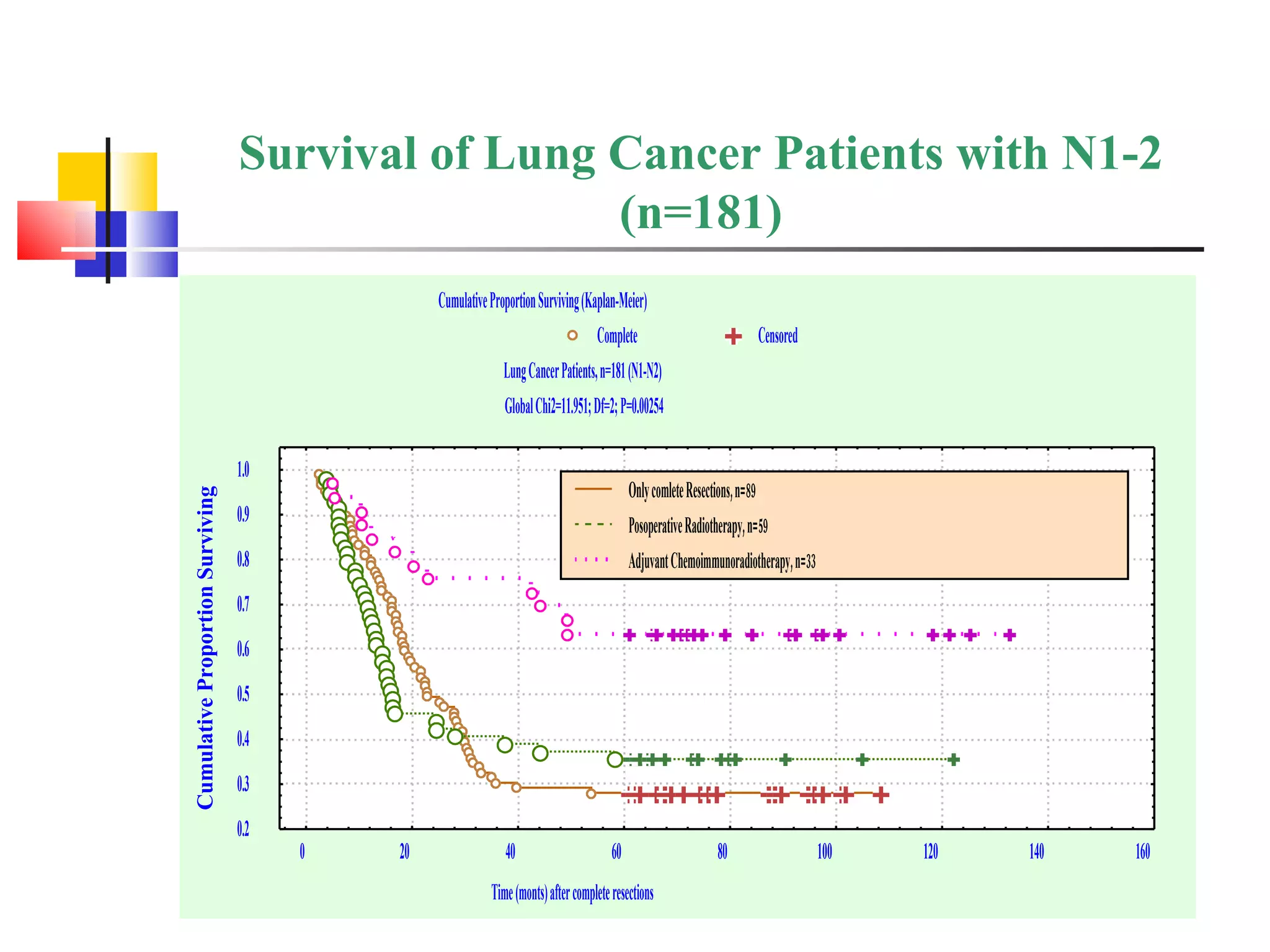
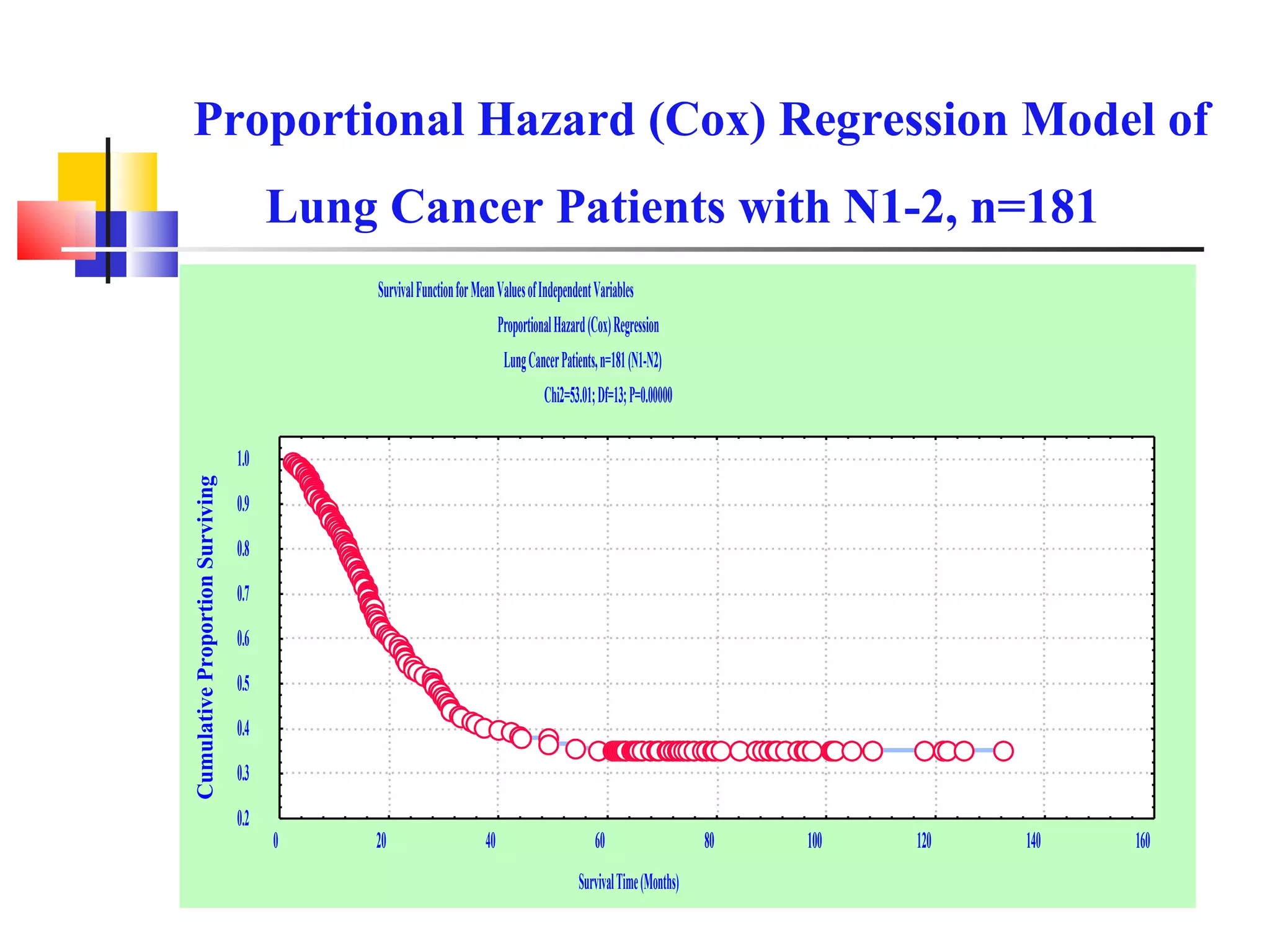
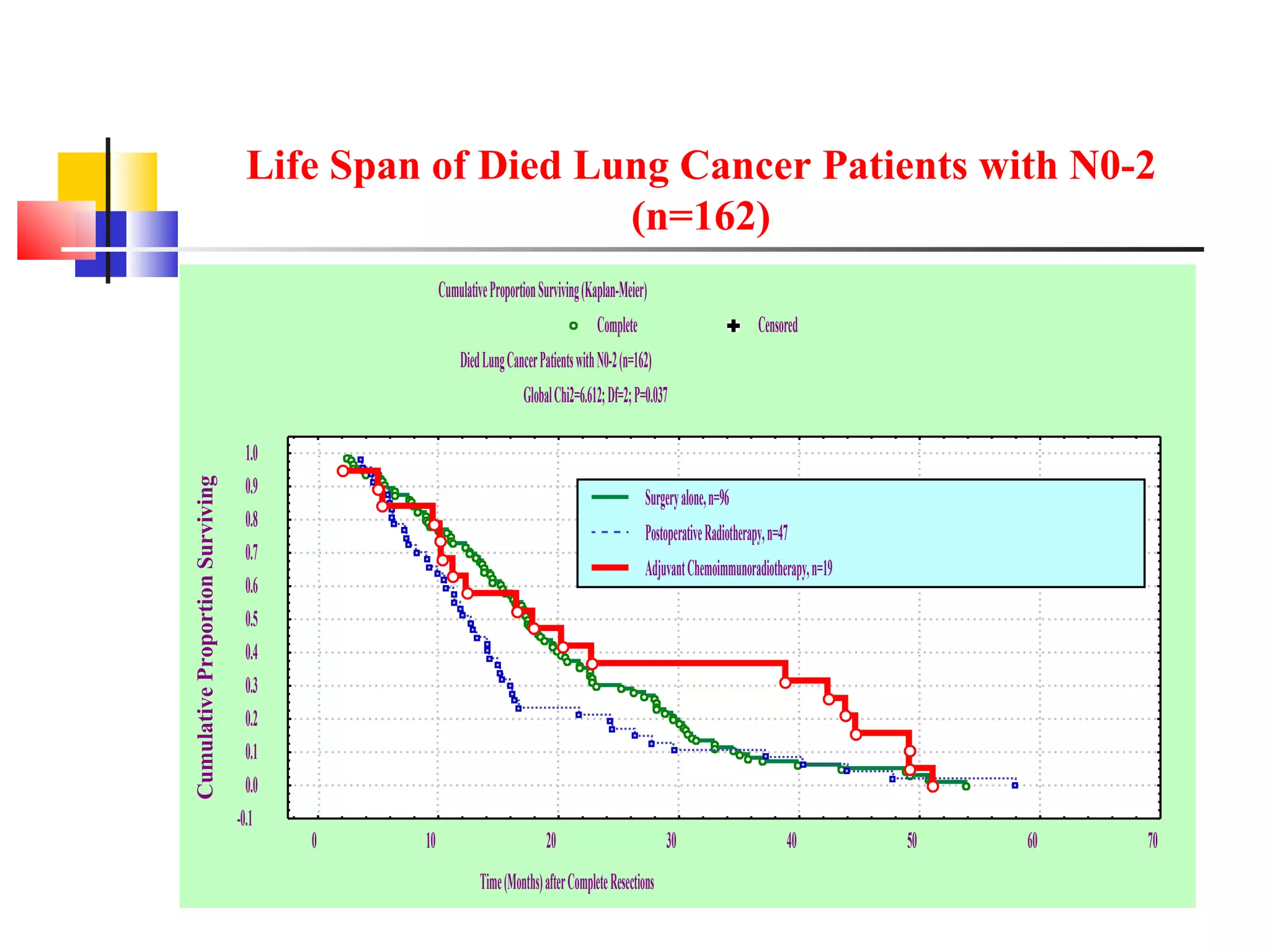
This document summarizes a study on the 5-year survival of non-small cell lung cancer patients after adjuvant chemoimmunoradiotherapy compared to surgery alone or postoperative radiotherapy. The study found that adjuvant chemoimmunoradiotherapy significantly improved 5-year survival and lifespan for patients with lymph node metastases (N1-2) compared to the other treatments. However, for patients without lymph node metastases (N0), the 5-year survival was not significantly different between adjuvant chemoimmunoradiotherapy and surgery alone or postoperative radiotherapy.


























































































