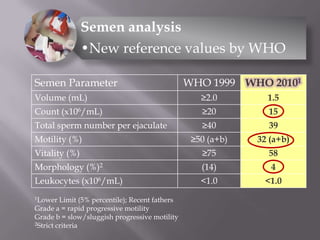
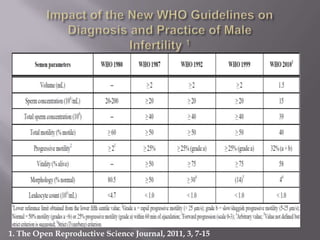
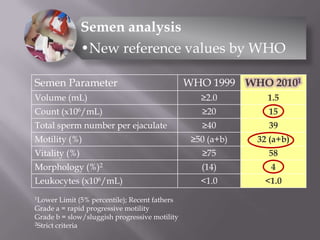
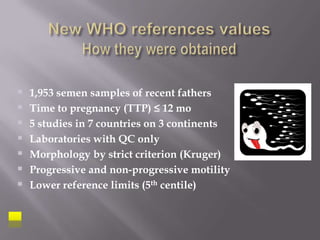
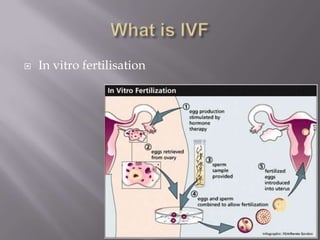
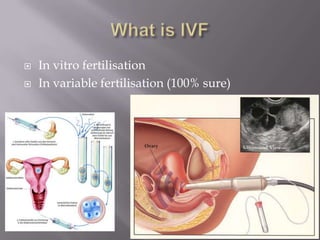
1. The document discusses new concepts in infertility including updated WHO reference values for semen analysis, the use of ICSI for male factor infertility, and success rates varying based on the cause of infertility.
2. ICSI, where surgically retrieved sperm are injected into eggs, has become an established procedure for couples with male subfertility to have a biological child, with reassuring post-natal outcomes reported so far.
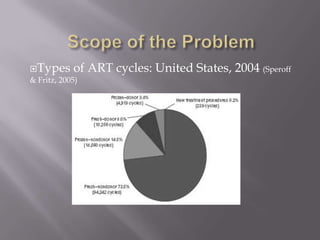
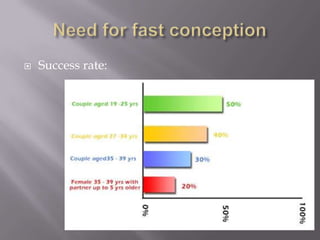
3. The success of IVF depends on the type of infertility, with male factor infertility seeing live birth rates around 40% and female factor infertility around 25%, higher than other causes of infertility.






















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









