Download as PDF, PPTX






















![Management
Parenteral iron therapy
Iron deficit Calculation:
• Ganzoni Equation:
Iron deficit [mg] = weight [kg] x ( target Hb - actual Hb g/dl ) x 2.4 + (500 to 1000)*
• Infed® Equation:
Iron deficit [mg] = LBW [kg] x ( target Hb - actual Hb g/dl ) x 2.21 + (13 x LBW [kg])*
• Schrier Equation:
Iron deficit [mg] = weight [kg] x ( target Hb - actual Hb g/dl ) x 2.145 + (500 to 1000)*
*for the repletion of iron stores](https://image.slidesharecdn.com/irondeficiencyanemia-240424123756-122d67f1/75/Iron-deficiency-anemia-IDA-Diagnosis-Management-2025-34-2048.jpg)
![Management
Parenteral iron can be given as IV or IM
• However, IM iron is not advised as it’s painful and stains the buttocks
Common parenteral iron therapy formula and concentration
Dose in mL = (Iron deficit [mg] + iron stores) / formula concentration (C)
Iron formula Concentration (C) Maximum / Single Infusion
Iron Dextran 50 mg/mL 1000 mg 1-4 hr
Iron Sucrose 20 mg/mL 300 mg 2 hr
Ferric Gluconate 12.5 mg/mL 250 mg 60 min
Ferumoxytol 30 mg/mL 1020 mg 60 min
Ferric Carboxymaltose 50 mg/mL 1000 mg 30 min](https://image.slidesharecdn.com/irondeficiencyanemia-240424123756-122d67f1/75/Iron-deficiency-anemia-IDA-Diagnosis-Management-2025-35-2048.jpg)



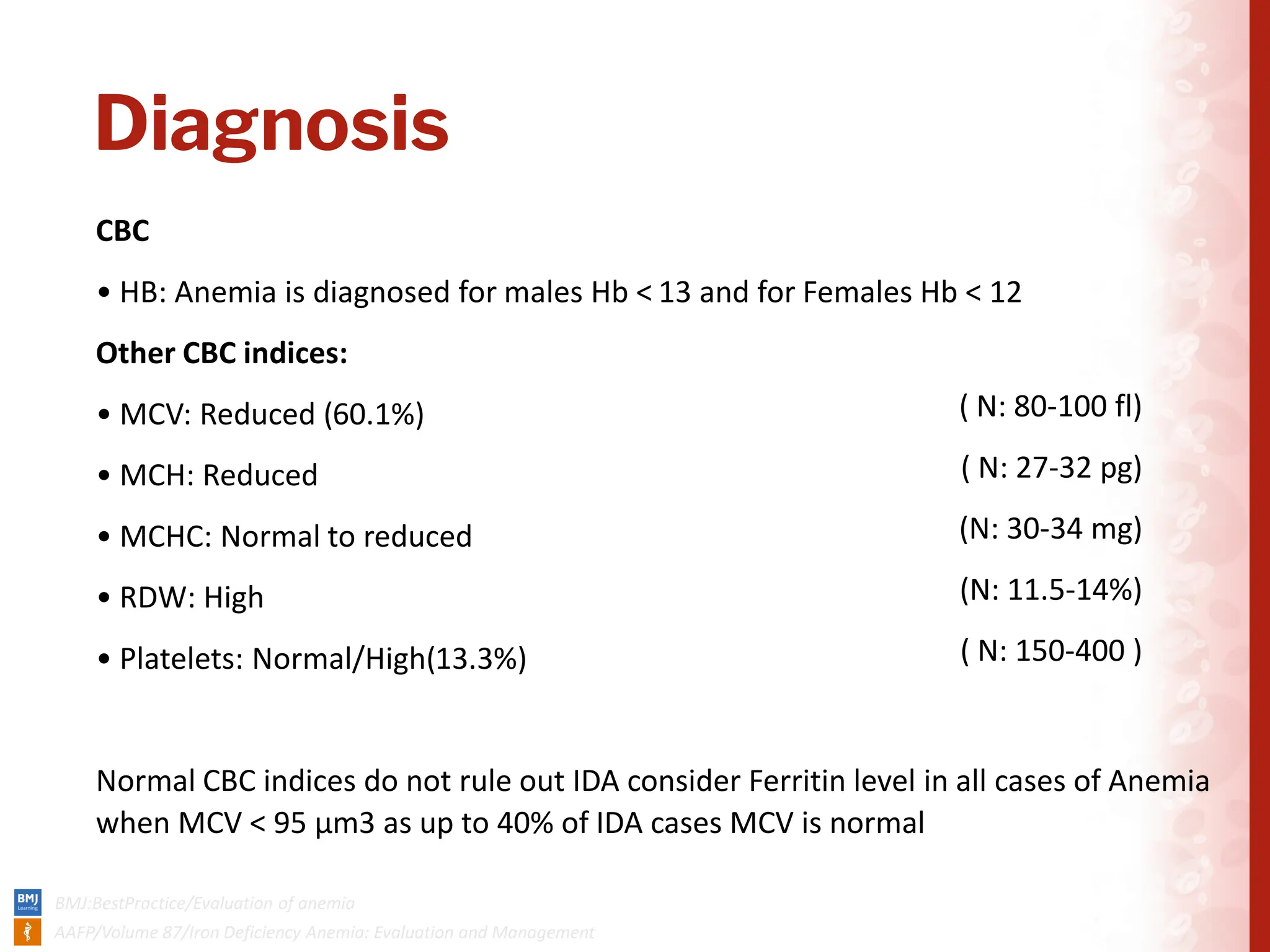
The document covers iron deficiency anemia (IDA), highlighting causes, clinical features, diagnosis, and management strategies. IDA, the most prevalent form of anemia globally, affects over 12% of the population, particularly women of childbearing age and children, and is diagnosed through specific blood tests such as ferritin levels. Management includes dietary changes, oral or parenteral iron therapy, and addressing any underlying causes, with recommendations for prevention and screening measures.






















































































