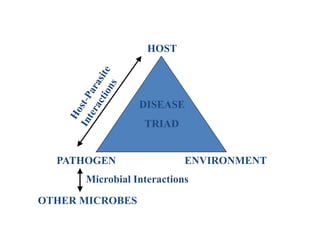
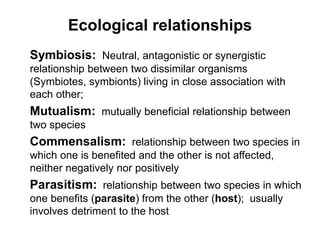
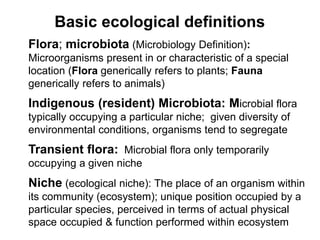
This document provides an introduction to the topics that will be covered in a microbiology course, including definitions, history, and branches of microbiology. It discusses the normal microbial flora of the human body and their ecological relationships. Key topics include the germ theory of disease, Koch's postulates, the miasma theory, and host-pathogen interactions. The course will cover bacteria classification and structure, growth, pathogenicity, sterilization methods, staining techniques, and examining various clinical specimens.


![HOST DEFENSE MECHANISMS
EXTERNAL (PRIMARY): Physical barrier of gross
surface area; e.g., skin, respiratory tract, gastrointestinal
tract, genitourinary tract
Mechanical and Physical Factors: sweat, fatty acids,
pH, indigenous competitive flora (microbial
antagonism), peristalsis, hair, cilia, urinary flushing,
mucus, [tears, nasal secretions, saliva (lysozyme)],
semen (spermine), mucosal secretory antibody (IgA
predominant)](https://image.slidesharecdn.com/introductiontomicrobiology-230404134134-c856f30b/85/Introduction-to-Microbiology-pptx-84-320.jpg)































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





