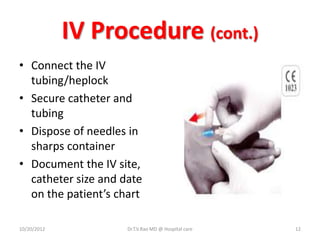
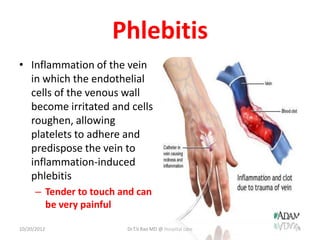
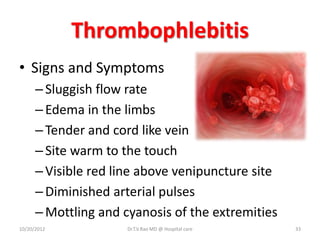
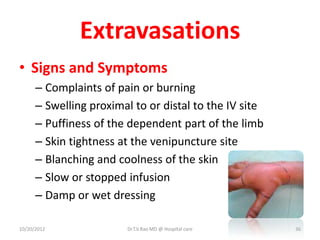
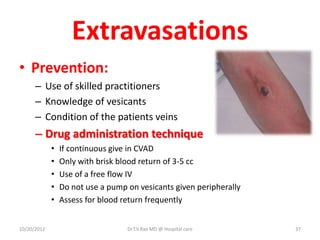
Intravenous (IV) medication administration involves inserting a catheter into a vein to deliver fluids, medications, or collect blood. Potential complications include local issues like hematomas at the insertion site or systemic problems like thrombosis blocking the catheter. Proper insertion technique and ongoing monitoring can help prevent complications. Signs like swelling, pain, or slowed infusion rates may indicate issues like phlebitis (vein inflammation) or extravasation of fluids outside the vein. Healthcare workers must take precautions like following needle safety procedures to avoid accidental needle sticks which can expose them to bloodborne diseases.





































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










