Download to read offline












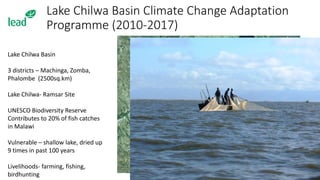


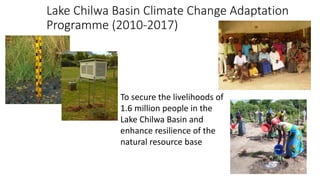









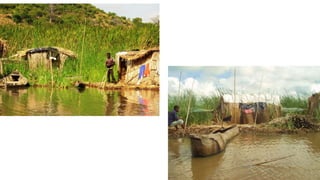

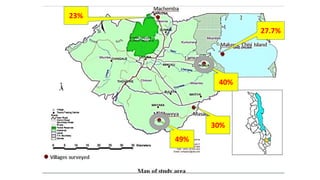
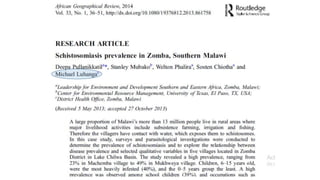


















The document discusses the Lake Chilwa Basin Climate Change Adaptation Programme (2010-2017) aimed at enhancing the resilience of 1.6 million people while addressing issues related to schistosomiasis (bilharzia), a neglected tropical disease prevalent in Malawi. It highlights the risk of increased schistosomiasis infections due to irrigation projects and the importance of incorporating disease control in climate change initiatives. The Sustainable Futures in Africa network emphasizes the importance of locally specific approaches to avoid unintended consequences of development projects.
























































