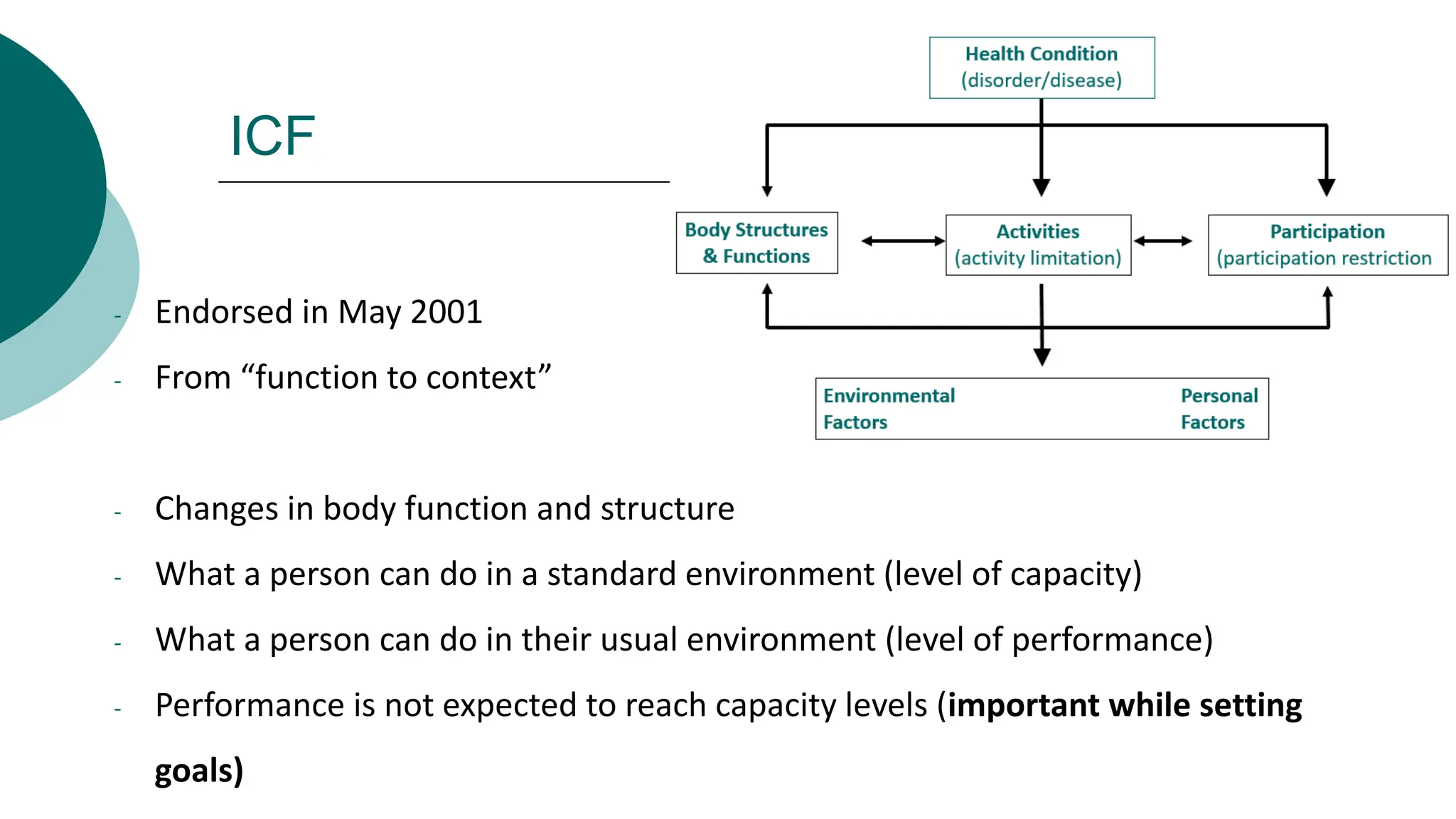
The document discusses the International Classification of Functioning, Disability and Health (ICF) framework. It provides an overview of the ICF's historical context and foundations. The ICF aims to provide a universal model of disability that considers functioning at the body, individual, and societal levels across the lifespan. It represents an interactive and integrative approach that considers both personal and environmental factors. The ICF can be used to guide clinical reasoning, documentation, goal setting, and outcome measurement in rehabilitation.




















































































![Needle examination [DOC 1 v2].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/needleexaminationdoc1v2-220917013003-7b2a4566-thumbnail.jpg?width=640&height=640&fit=bounds)



















