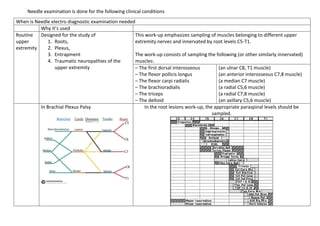
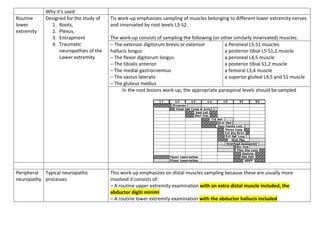
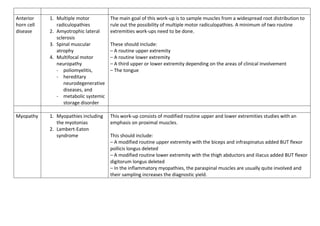
This document discusses different types of needle electromyography (EMG) examinations and their purposes. A routine upper extremity examination samples specific muscles innervated by cervical and thoracic nerve roots to study roots, plexuses, entrapments and traumatic neuropathies. A routine lower extremity exam similarly samples leg muscles. Peripheral neuropathy exams emphasize distal muscles. Anterior horn cell disease exams sample widespread muscles to rule out multiple radiculopathies. Myopathy exams focus on proximal muscles. Exams for neuromuscular transmission defects previously used repetitive nerve stimulation but now rely more on single fiber EMG for its greater sensitivity in detecting jitter, which represents variability in neuromuscular transmission.
![Neuromuscular
Transmission
Defects in neuromuscular
transmission
1. Myasthenia gravis,
2. Lambert-Eaton
syndrome,
3. Botulism
4. Many drugs and
anesthetic agents
also affect
neuromuscular
junction and impulse
transmission to elicit
their effects.
Above conditions result in
muscle weakness and
paralysis
Single fiber EMG has greatly altered the traditional neuromuscular transmission
defects work-ups by needle electrodes.
Through moment to moment variation in the shape and amplitude of affected
motor unit potentials is helpful, jitter analysis by single fiber EMG is a much
more sensitive means to study defects in neuromuscular transmission.
The technique requires the use of a special needle electrode which has a 25 µm
tip on a side port to allow recording from single muscle fibers. When the tip is
positioned in the vicinity of two muscle fibers belonging to the same motor unit,
two potentials are seen firing synchronously
In neuromuscular transmission disorders, the jitter is increased early in the
course of the illness, before repetitive stimulation tests become positive. In the
later stages, impulse blocking due to total failure in neuromuscular transmission
is seen and results in the disappearance of one of the potentials on the screen.
If, by means of a delay line and a signal trigger, one of them is made to trigger the
sweep, the distance between the two potentials, or interpotential interval, is
observed to vary from discharge to discharge. The distance between the first and
second potential is measured over a certain number of tracings and the mean
interpotential interval is calculated. The standard deviation around that mean or
the mean of the consecutive differences (MCD) are used in expressing the jitter
which to a large extent represents the variability in neuromuscular transmission.
[Not needed; only if you can remember]](https://image.slidesharecdn.com/needleexaminationdoc1v2-220917013003-7b2a4566/85/Needle-examination-DOC-1-v2-pdf-4-320.jpg)























































