
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Injury nutrients
Similar to Injury nutrients (20)
More from JA Larson
More from JA Larson (20)
Recently uploaded
Recently uploaded (20)
Injury nutrients
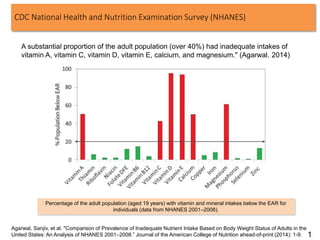
- 1. CDC National Health and Nutrition Examination Survey (NHANES) A substantial proportion of the adult population (over 40%) had inadequate intakes of vitamin A, vitamin C, vitamin D, vitamin E, calcium, and magnesium." (Agarwal. 2014) Percentage of the adult population (aged 19 years) with vitamin and mineral intakes below the EAR for individuals (data from NHANES 2001–2008). Agarwal, Sanjiv, et al. "Comparison of Prevalence of Inadequate Nutrient Intake Based on Body Weight Status of Adults in the United States: An Analysis of NHANES 2001–2008.” Journal of the American College of Nutrition ahead-of-print (2014): 1-9. 1
- 2. U.S. Department of Agriculture (USDA) 1. 93% = inadequate intake of vitamin E. 2. 56% = inadequate intake of magnesium. 3. 44% = inadequate intake of vitamin A. 4. 31% = inadequate intake of vitamin C. 5. 14% = inadequate intake of vitamin B6. 6. 12% = inadequate intake of zinc. 7. 8% = inadequate intake of folate. https://www.ars.usda.gov/SP2UserFiles/Place/80400530/pdf/0102 usualintaketables2001-02.pdf 2
- 3. 3
- 5. Admiral Nelson 11 March 1804 to Dr. Mosely: “The greatest thing in all military service is health; and you will agree with me that it is easier for an officer to keep men healthy than it is for a physician to cure them”. • BCT (CHPPM)(now USAPHC) – Males: 19-37% are injured in a 9-wk cycle – Females: 42-67% are injured in a 9-wk cycle • Most injuries are overuse, compared to traumatic – Males: 75% – Females: 78% • Most injuries involve the lower extremity (low back, pelvis, hip and leg)* – Males: 83% – Females: 87% • Activities associated with injuries in BCT – Weight bearing activity; predominantly running, marching, walking 5
- 6. Reducing Stress Fracture in Physically Active Military Women, Subcommittee on Body Composition, Nutrition, and Health of Military Women, Committee on Military Nutrition Research, Food and Nutrition Board, Institute Of Medicine, National Academy Press, Washington, D.C. 1998 • Ensure ”adequate energy and nutrient intakes to reflect the needs of the body at a moderate activity level (2,000-2,800 kcal/d) . • Put “nutritional labeling of all dining hall menu items and provision of food selection guidelines to women in garrison.” • “develop aggressive education programs for military women aimed at helping them identify and select appropriate foods and fortified food products to increase the number of women meeting their requirements for these nutrients.” • “If nutrition education and counseling sessions fail to promote increased intakes, the use of calcium-fortified products becomes essential.” • “Calcium supplements should be recommended under appropriate guidance by the military to meet women's special needs.” National Academy of Sciences Recommendations for Military Women: 6
- 7. 1. Calcium balance is compromised: Calcium (Ca) deficient diet upon BT entry: a. Minimum recommended (NAS IOM) 14-18 y/o 1,300 mg/day 19-30 y/o 1,000 mg/day b. Average Ca intake 19 – 30 yrs 600-700 mg/day c. Median Ca intake of women during BT 700-900 mg/day 2. High Ca losses occur in sweat during strenuous activity. Athletes lose 1 gm/day in sweat. (Study with collegiate basketball players Klesges, et al. 1996) 3. Recruits below age 30 have not achieved peak bone mass and require a positive Ca balance for bone gain. (maximize peak bone mass). 4. Intense training stimulates bone formation, increasing Ca demands (maximize bone adaptation). Micro-fracture repair is dependent upon Ca availability (maximize repair process) 5. 5,200 female U.S. Navy recruits, ages 17 to 35, doing eight weeks of basic training. 6. 2,000 mg Ca and 800 I.U. of Vit D/day (Oscal plus D) 7. Supplement Control group suffered 20 percent fewer stress fractures than the Control group . Navy Calcium-D Study (decreased stress fractures by 20%) Caution: Bones need 20+ nutrients, not just calcium 7
- 8. USARIEM BCT Female Iron and B-vitamin Deficiencies • 1993 study of 174 women in an all-female 8-week BCT company at Fort Jackson, SC (158 graduated). • Serum ferritin (body iron stores) were low pre-BCT (56% females at less than 20 ng/ml iron) and decreased further by graduation (84%)(pg.109). • Anemia was correlated with poor PT performance (pg. 111) • Serum folate levels were low normal pre-BCT and “decreased significantly over BCT.” (pg. 2) • Maternal low folate intake and blood levels have been "associated with (fetal) neural tube defects“ (pg. 39) (note: neural tube defects can be fatal for the fetus). • Menu was adequate in energy, but inadequate in B6, folic acid, calcium, magnesium, iron, and zinc. “Health, Performance, and Nutritional Status of U.S. Army Women during Basic Combat Training.” (1995)(ADA302042) NOTE: Study BCT menu governed by the 1985 AR 40-25 8
- 9. BCT Female Iron and B-vitamin Deficiencies 2001 AR 40-25 • Established iron MRDI at 10 mg/day for men and 15 mg/day for women. • Added notes that the MRDIs for iron, calcium, phosphorous, and magnesium are low for 17-18 year-olds and menus should be adjusted if the dining facility has a large <19 y/o population. (page 6, Table 2-1, Notes 9-12) NOTE 1: IOM standards for menstruating women on a regular diet are 18 mg/day of iron (27 mg/day for vegetarians) while men need 12 mg/day. Excess iron is not desirable. NOTE 2: Federal dietary policy shifted between 1985 and 2001. The 1985 policy was the ‘minimum needed to avoid disease’ while today’s policy is to ‘optimize health.’ 9
- 10. • Separate review of multiple studies. • 17% of women were iron deficient (<12 ng/ml) and 8% were anemic at BCT entry. • 35% were deficient and 26% were anemic at AIT entry. Institute of Medicine (IOM) Review National Academy of Science’s Institute of Medicine (IOM) Committee on Military Nutrition Research (CMNR) 1995 “Review of Issues Related to Iron Status in Women During U.S. Army Basic Combat Training” 10
- 11. Institute of Medicine (IOM) 2006 Mineral Requirements for Military Personnel: Levels Needed for Cognitive and Physical Performance During Garrison Training, Committee on Mineral Requirements for Cognitive and Physical Performance of Military Personnel, Committee on Military Nutrition Research, ISBN: 0-309-65790-3, 512 pages, 6 x 9, (2006) http://www.nap.edu/catalog/11610.html Recommendations for Achieving Sufficiency Supplementation or fortification programs targeted specifically for women appear to be the only realistic approach for meeting women’s iron requirements during training periods, and especially in hot environments. Educational approaches used during garrison training should aim to increased meat intake so that heme iron in the diet is maximized. However, it is unlikely that food-choice alternatives can increase iron intakes to the > 20 mg/day range. Supplementation during pregnancy and fortification have been used effectively for decades. Research should be conducted to elucidate which approach will best meet women’s iron needs during military training (see Chapter 4, Research Needs). 11
- 12. Design: - 8-wk randomized, double-blind, placebo-controlled trial, Soldier volunteers (n = 219) were provided with an iron supplement or a placebo. - Iron status tests pre- and post-BCT. - Two-mile running time post-BCT. - Mood measured with the Profile of Mood States questionnaire pre- and post-BCT. Results: - Control Group iron levels were lowered post-BCT. - Iron supplementation: + Raised iron levels. + Improved vigor scores on the Profile of Mood States + Improved running time in women with iron deficiency anemia. Conclusions: - BCT lowers iron levels - Iron supplementation improves iron status. - Iron supplementation improves mood and physical. Army BCT Female Iron McClung et al, Randomized, double-blind, placebo-controlled trial of iron supplementation in female soldiers during military training: effects on iron status, physical performance, and mood. Am J Clin Nutr 2009;90:124–31. 12
- 13. Osteopenia Source: Dr. Rivero study at Great Lakes Naval Training Center (2001-2002). • High rates of osteopenia in stress fracture cases. • Women have higher rates of osteopenia and multiple stress fractures. 13
- 14. Screen (QUS) re Stress Fractures in Female Army Recruits• QUS calcaneal measurements on 4,139 female Army recruits at Basic Training (BT) start. • Stress fractures were 4.7%. • The highest risk of stress fracture was found in white women in Q1 of SOS who smoked and didn’t exercise (RR, 14.4). • QUS measurements plus evaluation of individual risk factors can identify recruits who are at the very highest risk of stress fracture. Lappe et al, Quantitative Ultrasound: Use in Screening for Susceptibility to Stress Fractures in Female Army Recruits, Journal of Bone And Mineral Research, Volume 20, Number 4, 2005 14
- 15. Navy Female Recruit Calcium and Vitamin D Study • Stress fractures occur in 0.2-5.2 % of male recruits and 1.6-21.0% of female recruits. • Calcium Balance is compromised − Ca deficient diet upon entry in BT. Minimum recommended Ca 1,000mg/d Average Ca intake 19 – 30 yrs 600-700mg/d Median Ca intake of women during BT 700-900mg/d − High Calcium losses occur in sweat during strenuous activity. Study with collegiate basketball players Klesges, et al. 1996. • Sample size: 2,803 • Treatment: − Randomized, Double Blind, Placebo Controlled − 2,000 mg Calcium & 800 IU Vit D • Results: 20% lower incidence of stress fractures 15
- 16. 16 1. Clinical Practice Guideline for Hip Pain. 2. Early effective management works: a. Avoids the fracture. b. 75% Increase in FNF detection 3. Ideally train Drill NCO & TMC medics to look for a rocking gait and hip pain. Source: CPT Short, MAH, FJ ATC Femoral Neck Fracture 1. Small numbers, but high costs. 2. 100% Medical Board. 3. Lifetime of treatment & surgeries. 16
- 17. • Treat Marines forward as Warrior Athletes. • Sports Medicine Physicians. • Certified Athletic Trainers (ATC’s) – Contracted civilians who work for USMC commands. – GREEN ASSETS (NCAA model) – Aligned with SMART rehab clinic operations – Clinically supervised by Navy Sports Medicine MDs when dealing with injuries – Emphasis on prevention, education, and treatment – Collect/enter injury data into TIMS (injury database) • 3 trainers for Parris Island (GIT)/1 ATC for San Diego. • 3 Athletic Training Room (ATRs) for Parris Island Fix Forward: USMC SMIP Athletic Trainer Initiative RESULTS + Increased Paris Island grad rate (female 68.3% to 74.7%) + Increase in BCT Return to Full Duty (RTFD) rates from rehab: + male 55.5% to 64.3% + female 37.5% to 52.2% + Increase in BCT recycle grad rates (female 63.5% to 75%). – Decrease in BCT rehab discharge rates (male 13%; female 24%) – Decreased musculo-skeletal discharges at Infantry School (see chart at left). – Decreased attrition at OCS − male 8.7% to 3.8% − female 18.1% to 5.9%) + Greater cadre knowledge + Critical feedback on sources of injuries leading to fixes. + Conservative estimate of $3.5M in cost avoidance and $2.9M in Return on Investment in FY04 vs FY03. 17
- 18. Pre-habilitation 1. Females are at risk for ACL injuries 2. Balancing quad-ham muscles reduces knee injuries by 80%. Pre-training Post-training Hewett et al. The Effect of Neuromuscular Training on the Incidence of Knee Injury in Female Athletes: A Prospective Study, THE AMERICAN JOURNAL OF SPORTS MEDICINE, Vol. 27, No. 6 Untrained Females Trained Females Males Injury Incidence/ 1,000 Player Exposures *p< .05 ACL Injury Prevention 18
- 19. Pre-BCT Training Programs are Effective 1. BLUF: The FTU PCU lowers overall discharge attrition by 500-800+ Soldiers (0.4-0.8+%), as well as lowers course attrition and injury rates. 2. 4%-7% of men and 10%-24% of women fail the RECBN 1-1-1 assessment historically. 50-75% of the PCU at GIT sites will be female. 3. PCU Results: a. Lower course attrition: In the “1-1-1 Fail No PCU” group, men are 2.5 times and women are 1.5 times more likely to attrit from BCT. b. Lower discharge attrition: In the “1-1-1 Fail No PCU” group, men are 3.0 times and women are 1.9 times more likely to be discharged from BCT. c. Lower injury rates. d. The USMA experimental PCU-X vice the traditional PCU improved female outcomes, but male outcomes were worse (but still better than no PCU). Recommendation is that USAPFS design a new PCU PT POI. e. Option: a 12 week BCT PCU company to maximize program flexibility, maintain bonding, provide non-PT training, get resourced, etc. Knapik et al, Increasing the Physical Fitness of Low-Fit Recruits before Basic Combat Training: An Evaluation of Fitness, Injuries, and Training Outcomes, Military Medicine, 171, 1:45, 2006 19
- 20. Control Group Standardized PT Program Week 1 Week 3 Week 5 Week 9 Time (in weeks) Injury Rates 33% decrease Injury Control USAPFS Standardized PT Program Good PT & workload progression design maintains/exceeds standards and lowers injury rates 20
- 21. • BCT grads arrived at AIT with high injury rates (approx. 28% men; 48% women). • PT running was the primary cause of musculoskeletal injuries. • Changing the running program • Reduced Clinic Visits - 36.5% • Reduced Profiles - 48.6% • No difference in APFT Scores • Reduced APFT retakes - 50% • Saved 612 limited duty days/week/BN AMEDDC&S Operation Aegis Injury Control If implemented at all IET/AIT sites: $9M/yr & 1.5M limited duty days/yr Potential Savings 21
- 22. 0% 20% 40% 60% 80% 100% 1994 1995 1996 1997 1998 1999 Uninjured 1,834 Injuries Prevented Injured Results for Army Basic Training: Injury 0% 20% 40% 60% 80% 100% 1994 1995 1996 1997 1998 1999 Training Successes Discharged 1,260 Discharges Prevented Results for Army Basic Training: Attrition Defence Injury Prevention Program (DIPP) Australian Department Of Defence 1. Reducing injuries reduced attrition: 70% reduction over 4 years in rates of injury and attrition 2. Gives CDRs the tools; harnesses Commander’s knowledge and skills working together to address their own injury problems. 3. 95% reduction in pelvic stress fracture rates in female recruits. 22
- 23. The Dark Side Attitudes 1. G1 Insist-Assist Study showed leaders‘ attitudes affected attrition rates (1984). a. “High Attrition Leaders” believe they were ‘gate guarders.’ b. “Low Attrition Leaders” believed they were developing Soldiers. 2. Emotional Events (‘high fear events,’ ‘food deprivation’, ‘sleep deprivation,’ ‘extreme PT,’ etc.) may be mis-perceived by some as preparing Soldiers for war, or strengthening them to cope with stress. 23
- 24. % 17-20 y/o Who Do Not Meet Army Accession Weight Standards Source: Nolte et al, “U.S. Military Weight Standards: What Percentage of U.S. Adults Meet the Current Standards?” The American Journal of Medicine, Vol 113, Oct 15, 2002 Obesity 24
- 25. IDENTIFY HAZARDS / ASSESSS HAZARDS / DEVELOP CONTROLS / IMPLEMENT CONTROLS / SUPERVISE-EVALUATE 15 Organizational Behavioral Health Physical Fitness Demographic FemaleAFQT IIIB Not Tier I Bonus Never thought about quitting High School Pre- accession Injury High BMI Low BMI High Initial Fitness Old >26 years Child- ren Entry Pay Grade African American Hispanic Hx shortness of breath Combat Arms MOS Hx backpain Hx chest pain Current smoker Hx depression Ever suspended /expelled Law Waiver Hx fainting Young <19 years Regular Army IET Attrition Risk Profile 12/23/09 25 • Base-case IET attrition risk is 15% • Further left or right of the center line means increased risk (or less risk) of attrition. • Bubble size is relative size of RA accessions that are associated with that factor. 20% female bubble is about 1/2 the size of the 33% TSC IIIB bubble. • Not Tier 1 (10%) • Female (20%) • AFQT IIIB (30%)