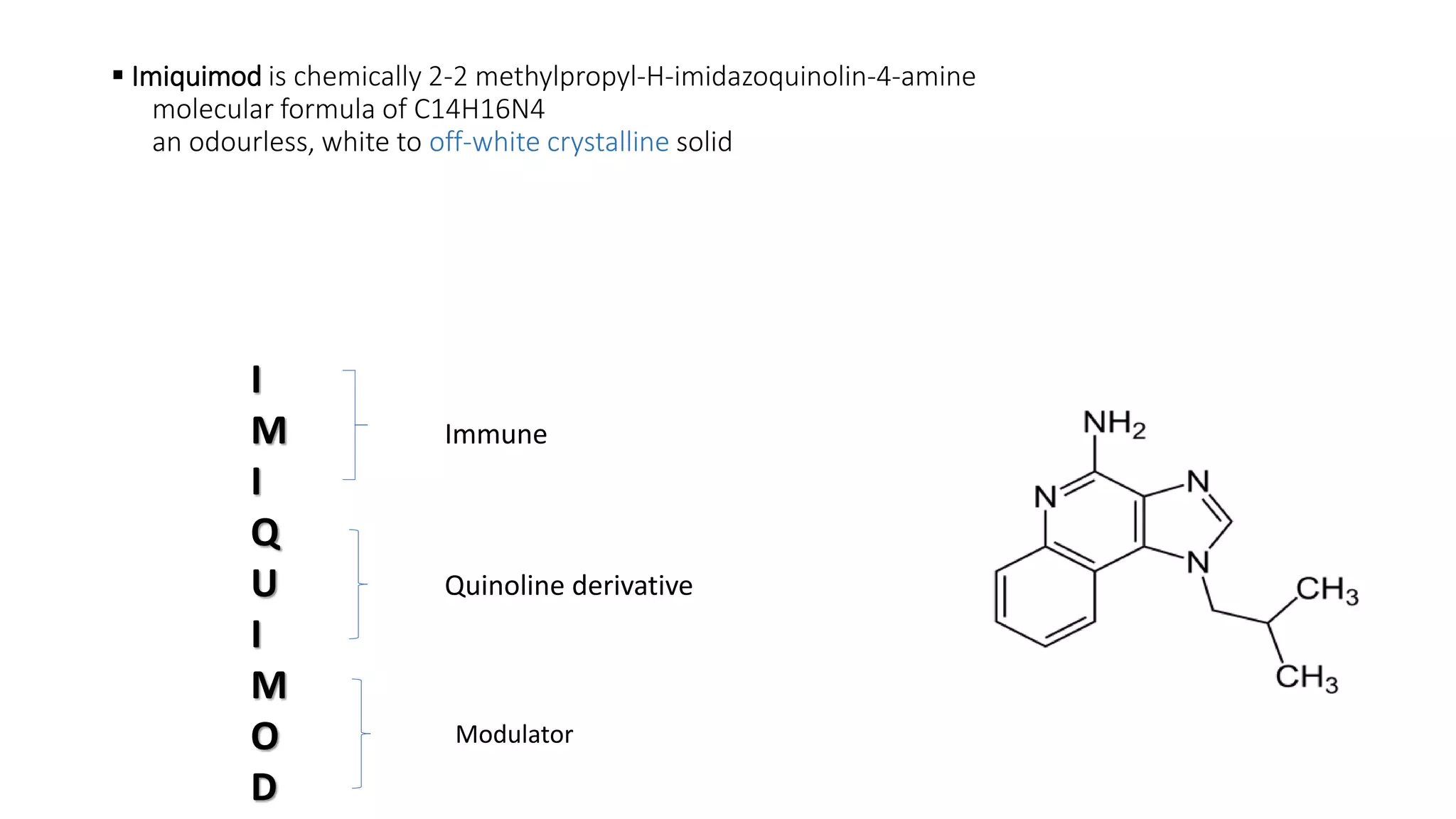
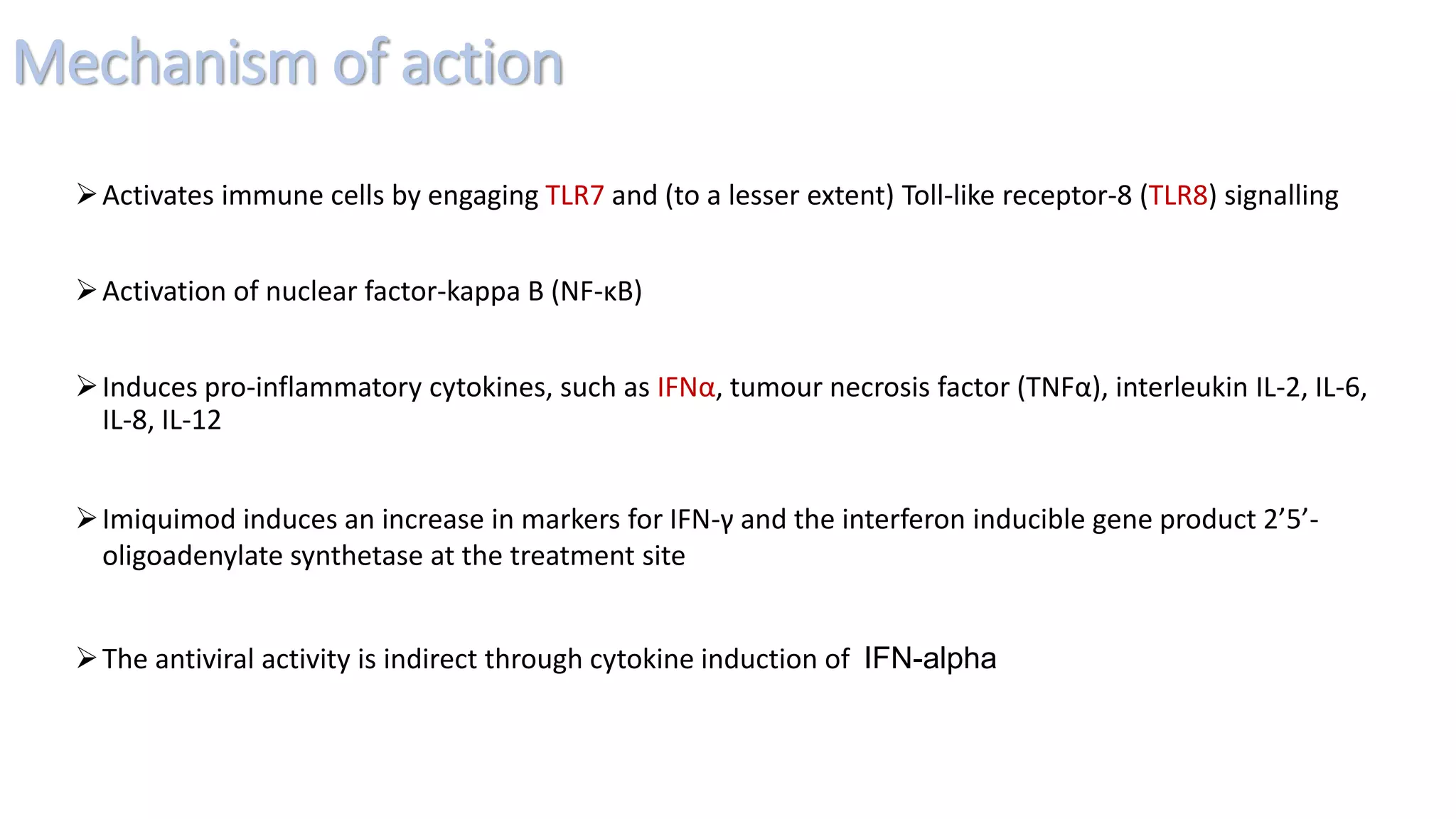
Imiquimod is a topical immune modulator used in dermatology, approved for treating external genital warts, actinic keratoses, and superficial basal cell carcinoma. It works by activating immune cells and inducing pro-inflammatory cytokines, but is contraindicated in known hypersensitivity and children under 12, and care should be taken during pregnancy and lactation. Clinical studies indicate varying efficacy rates, with ongoing research needed to explore its potential for other dermatological conditions.