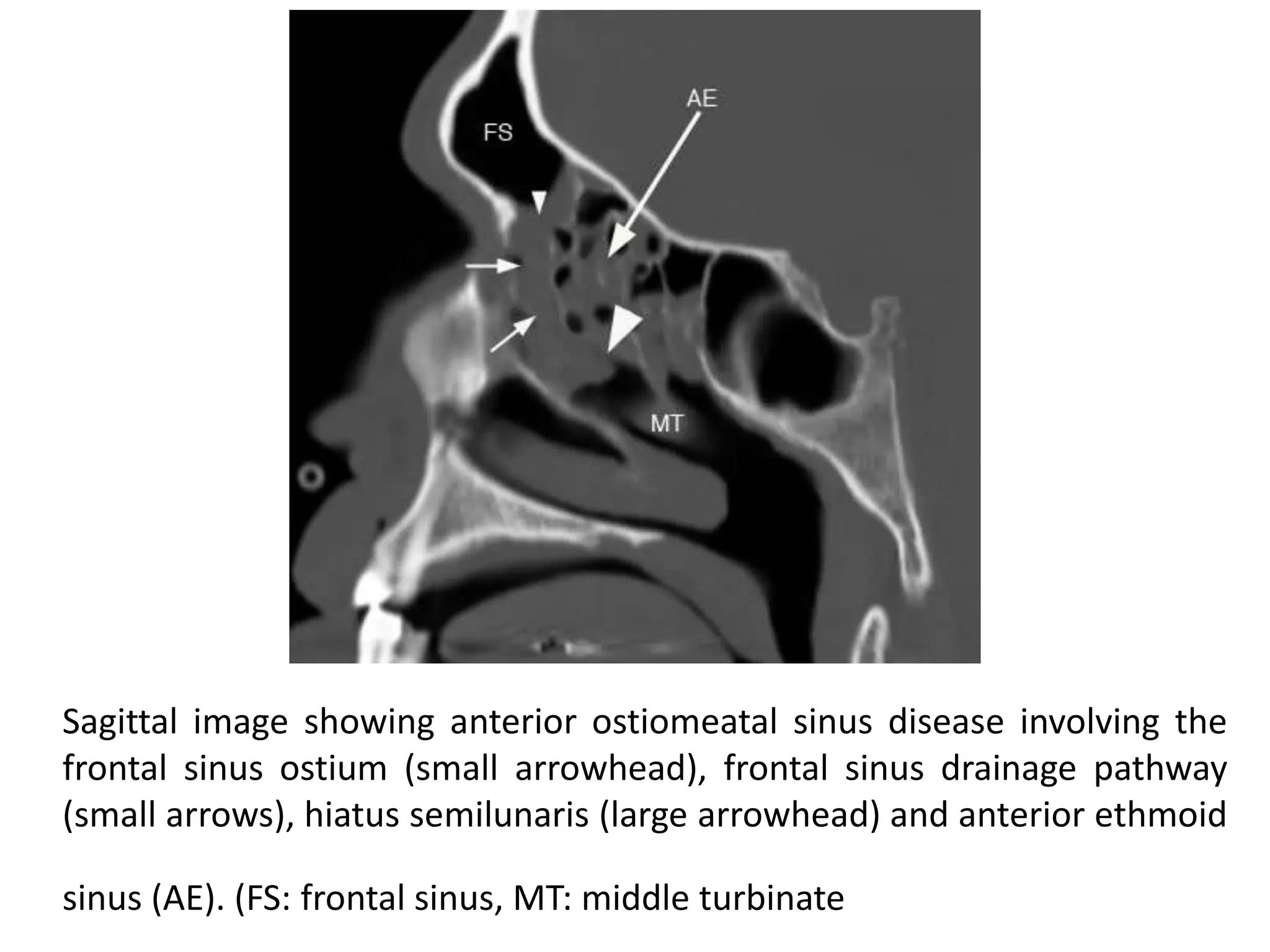
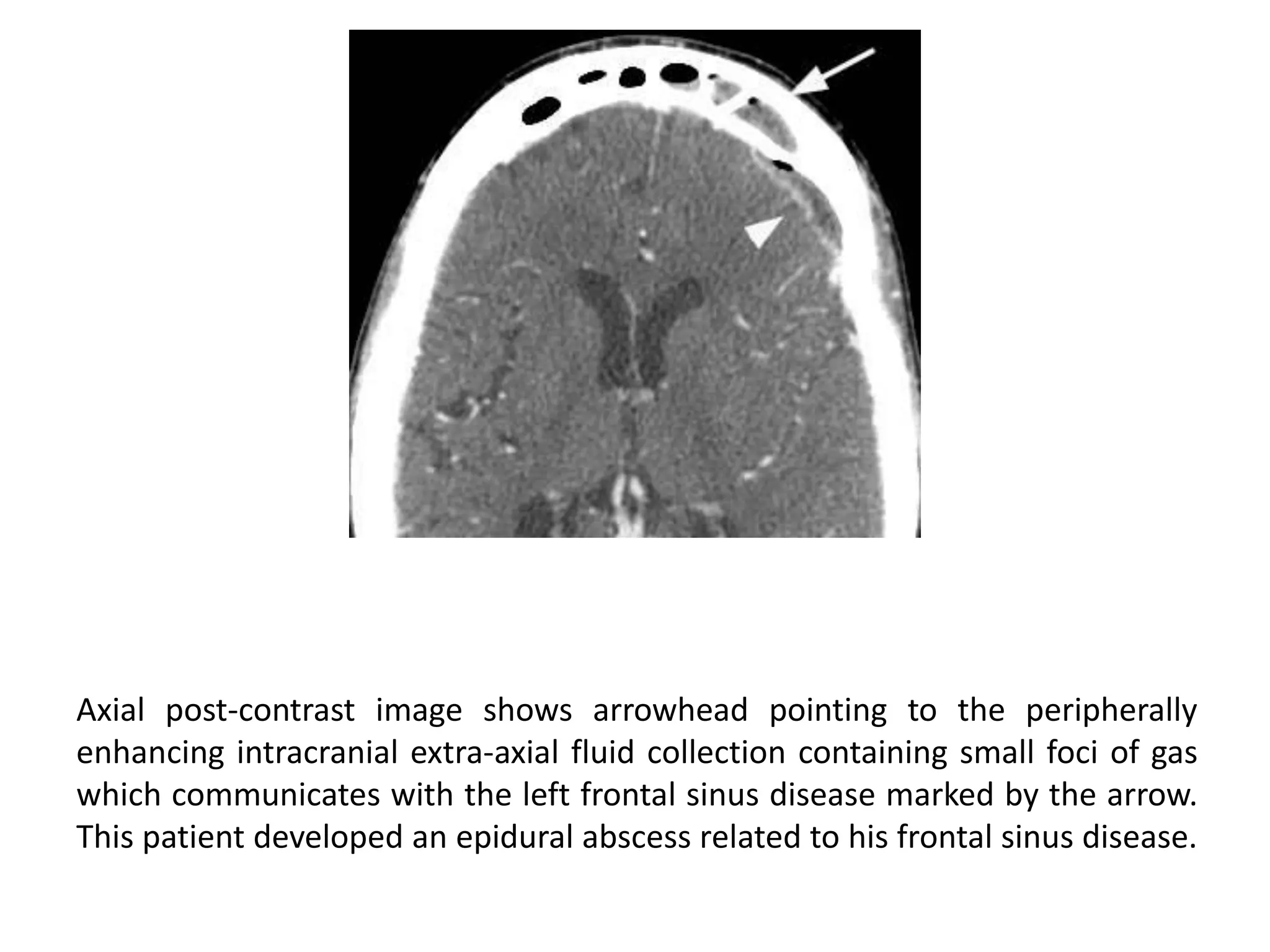
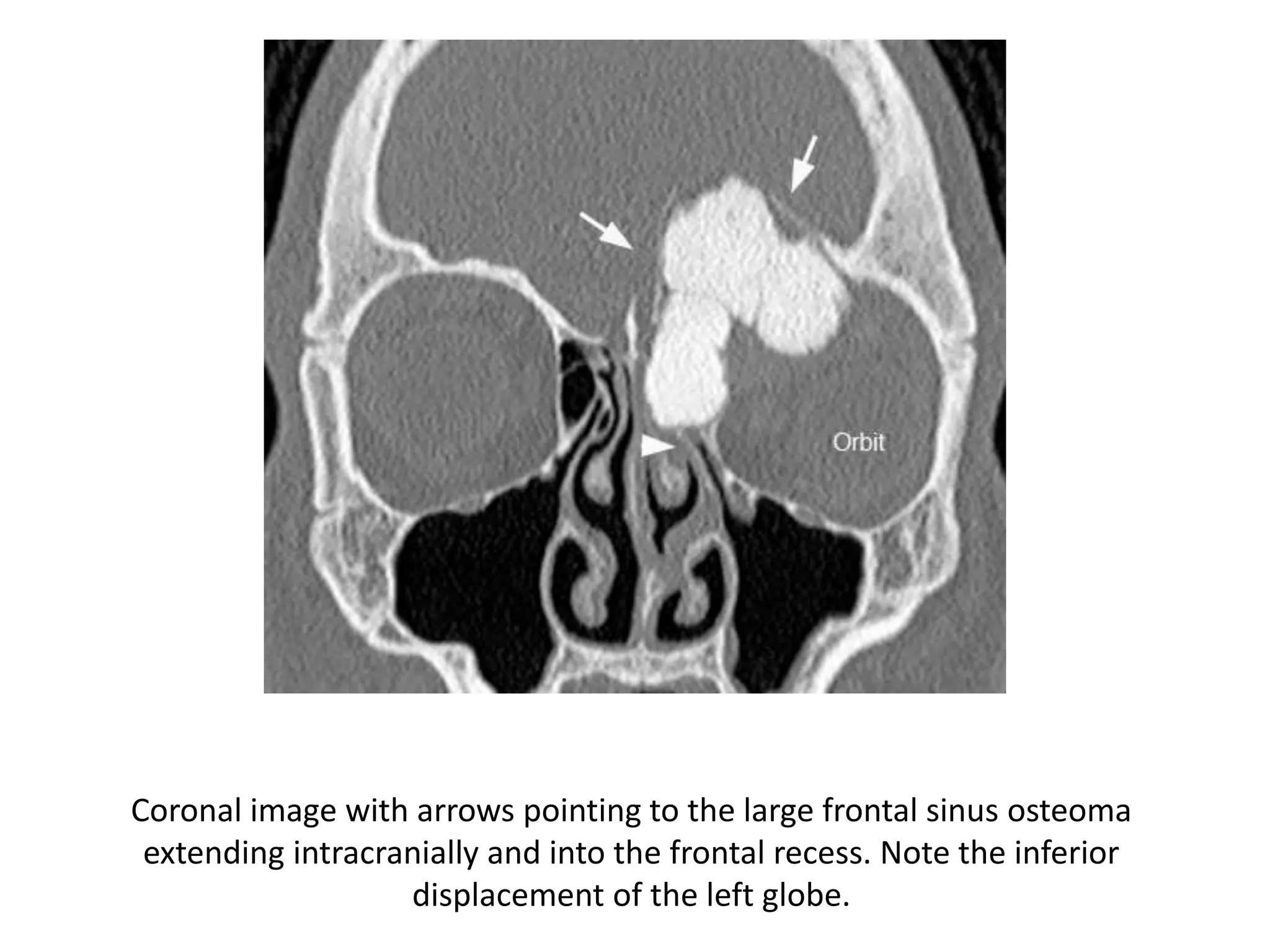
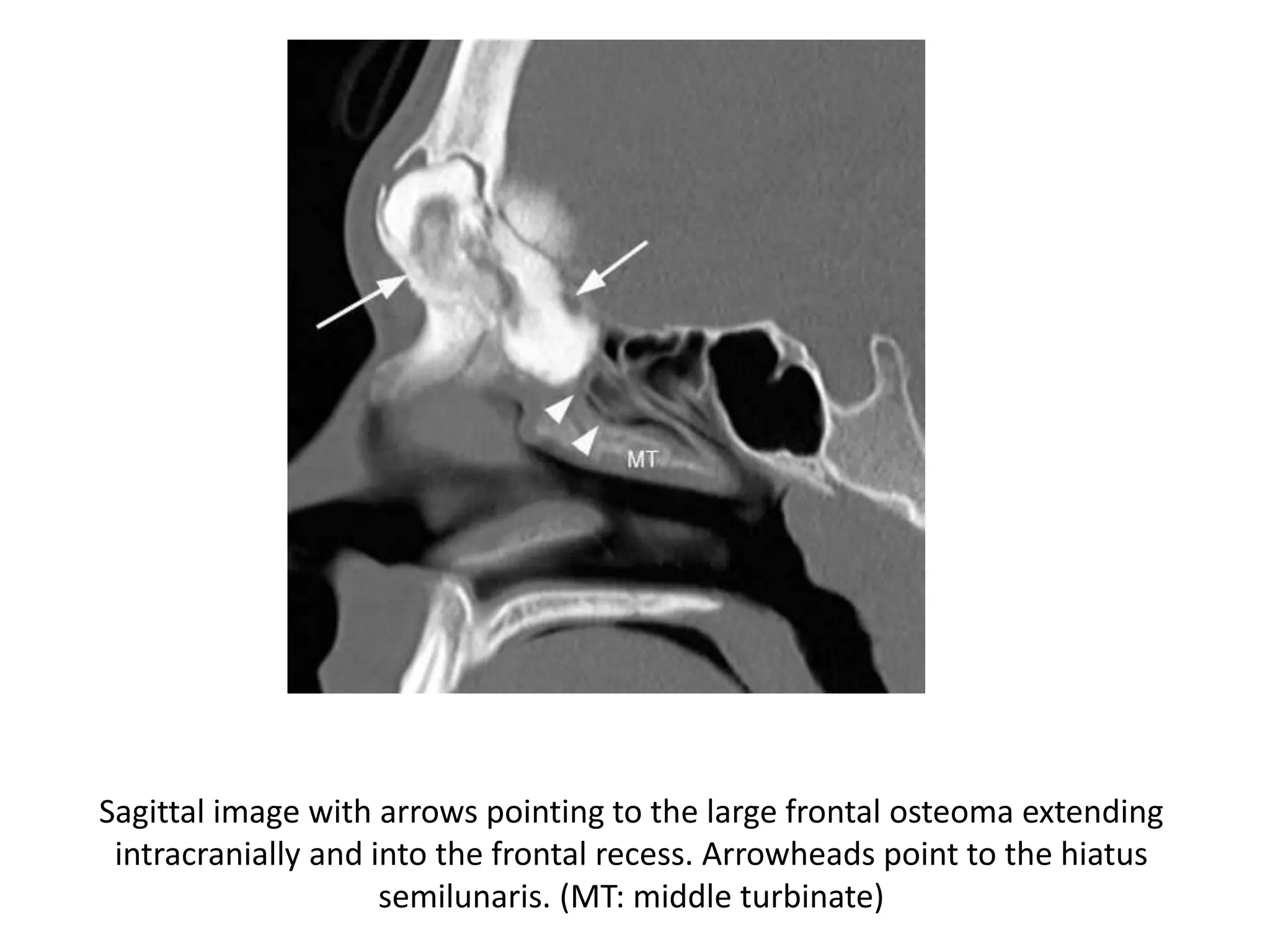
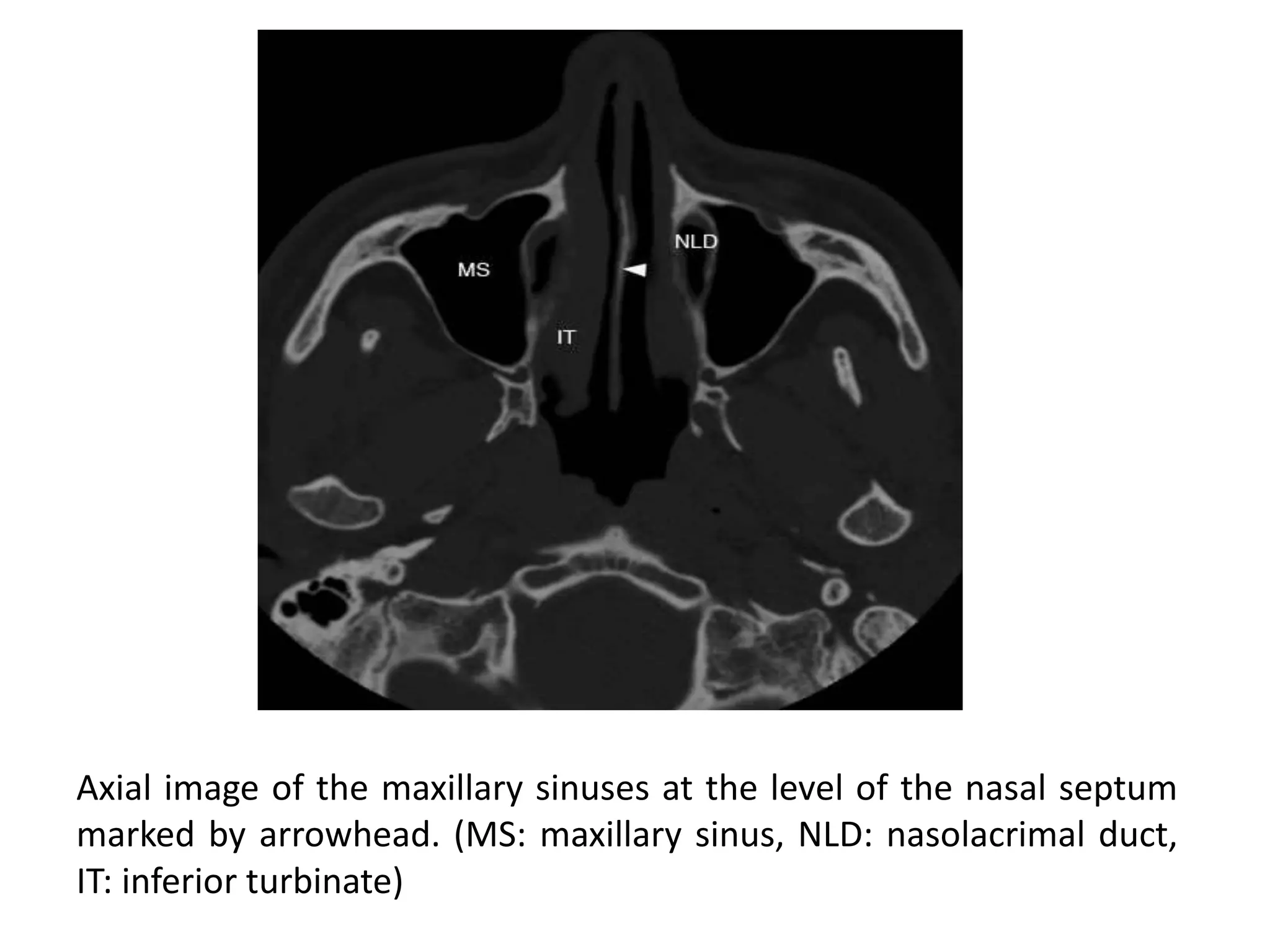
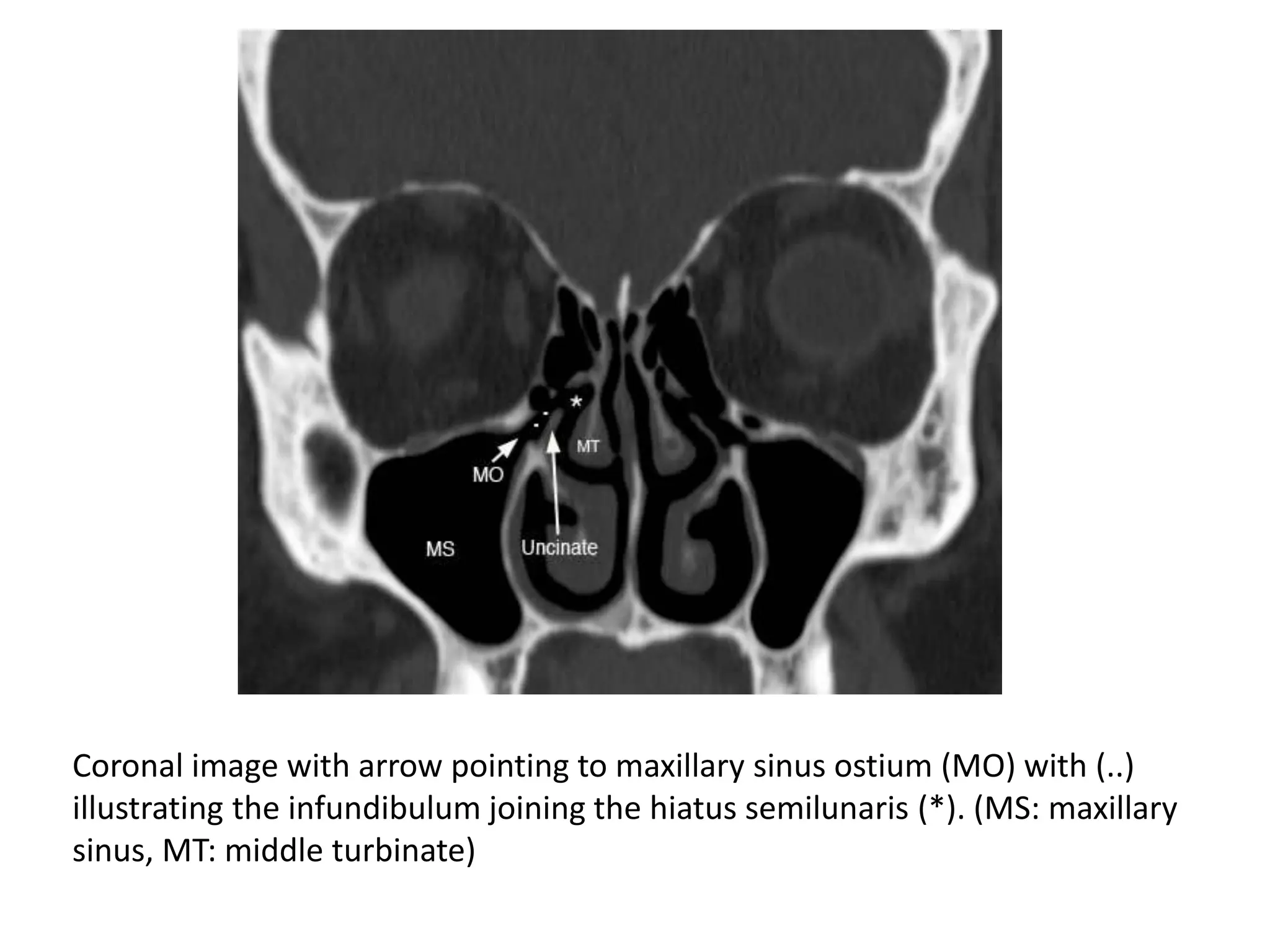
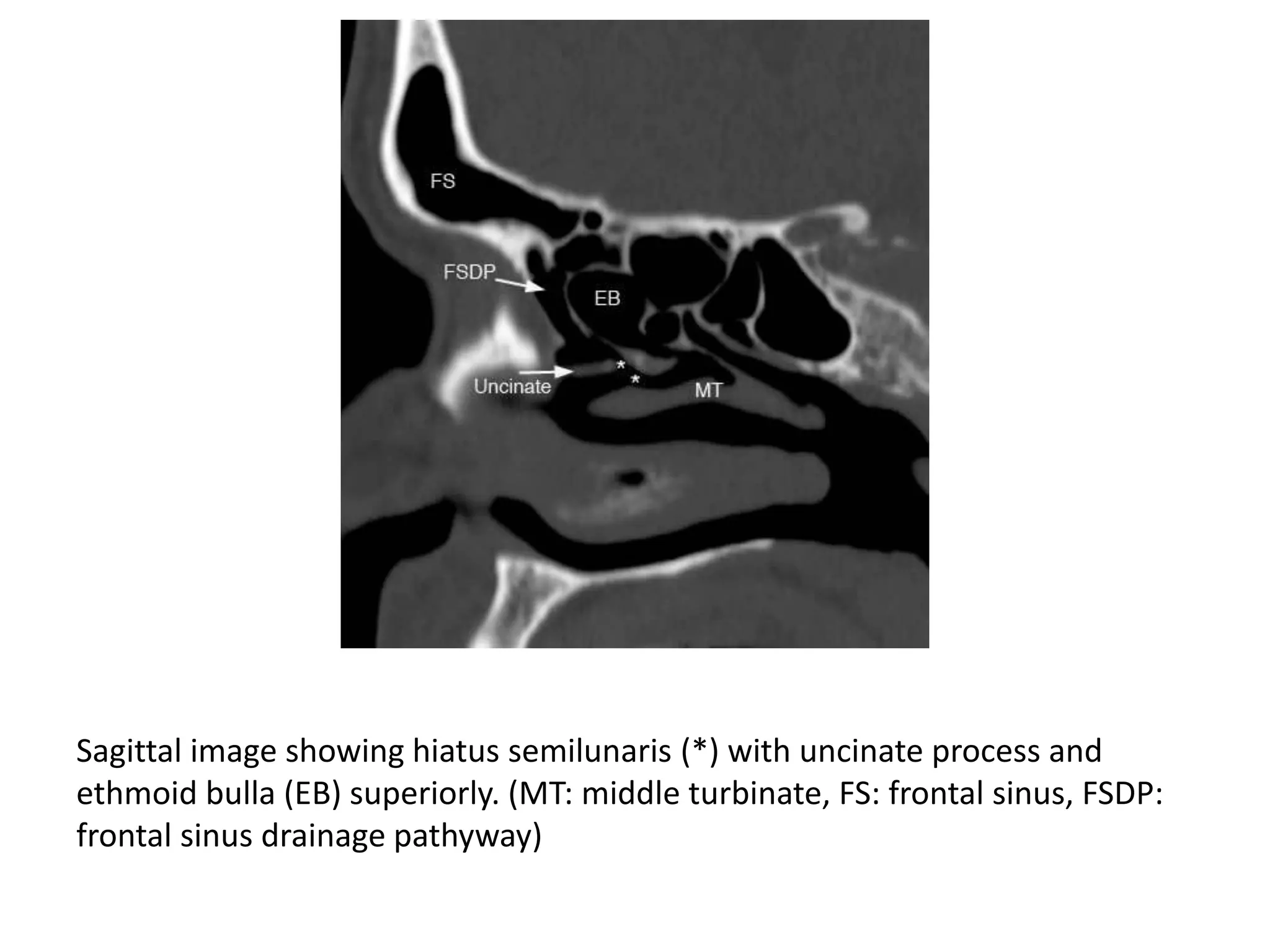
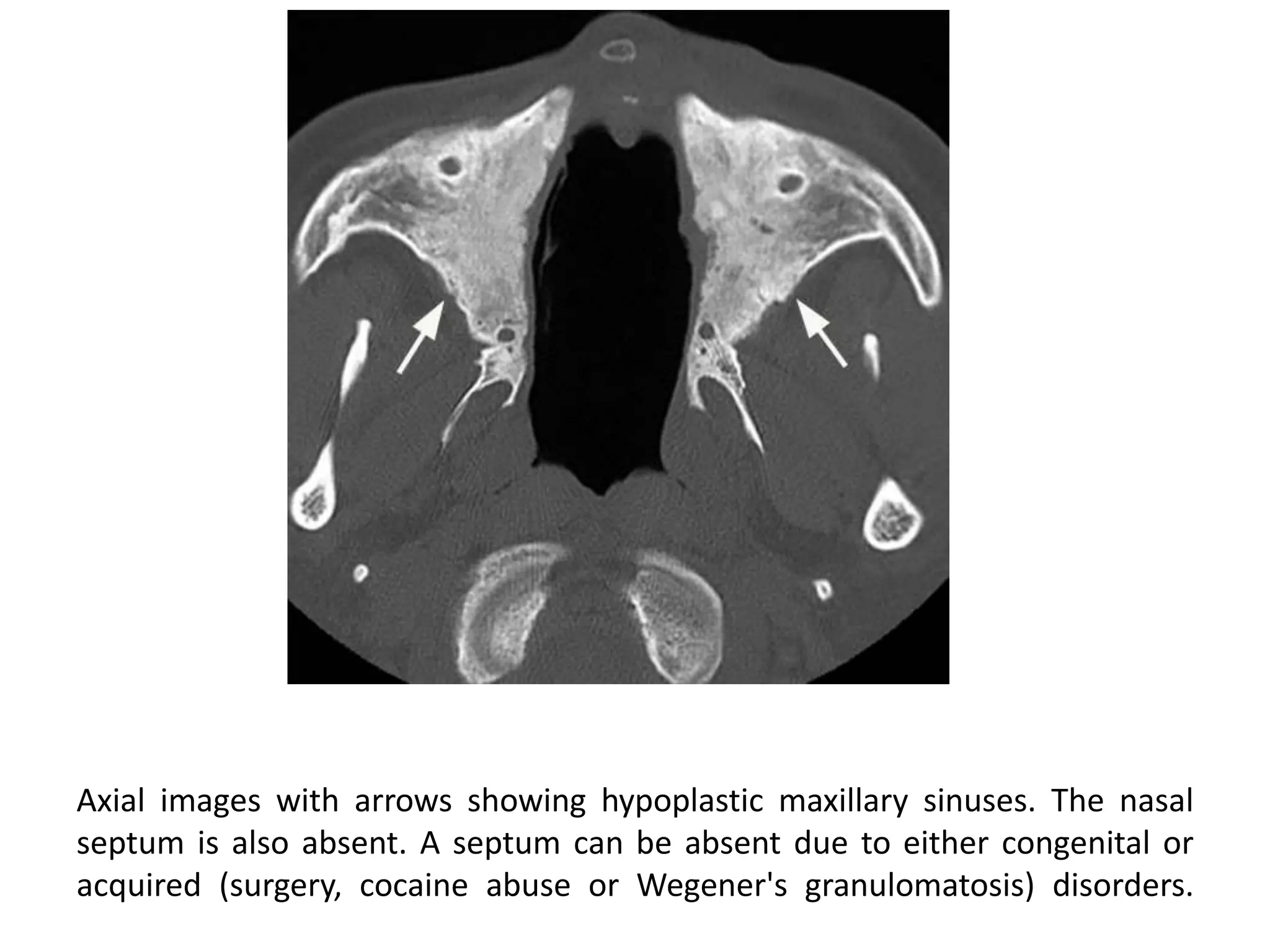
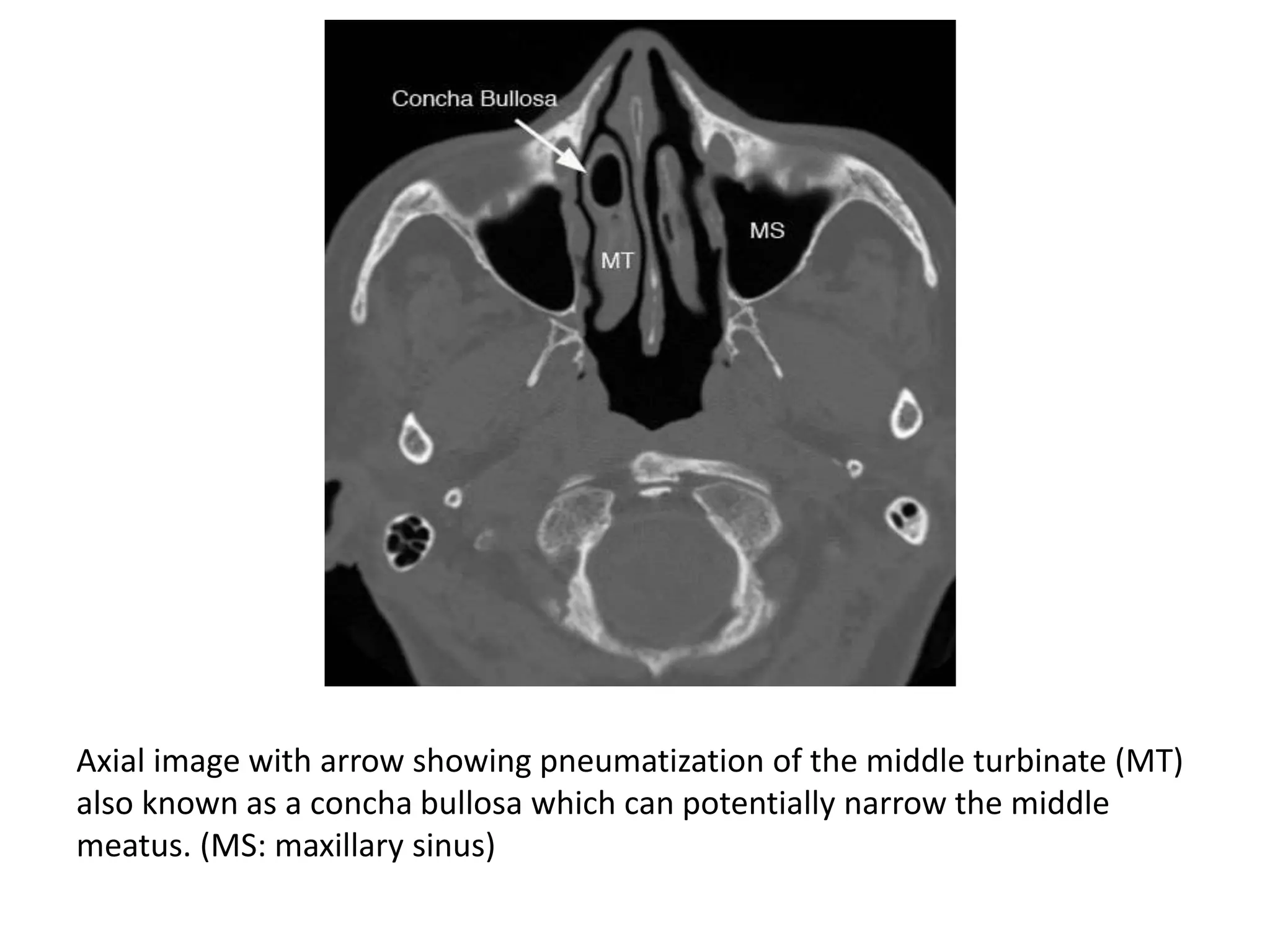
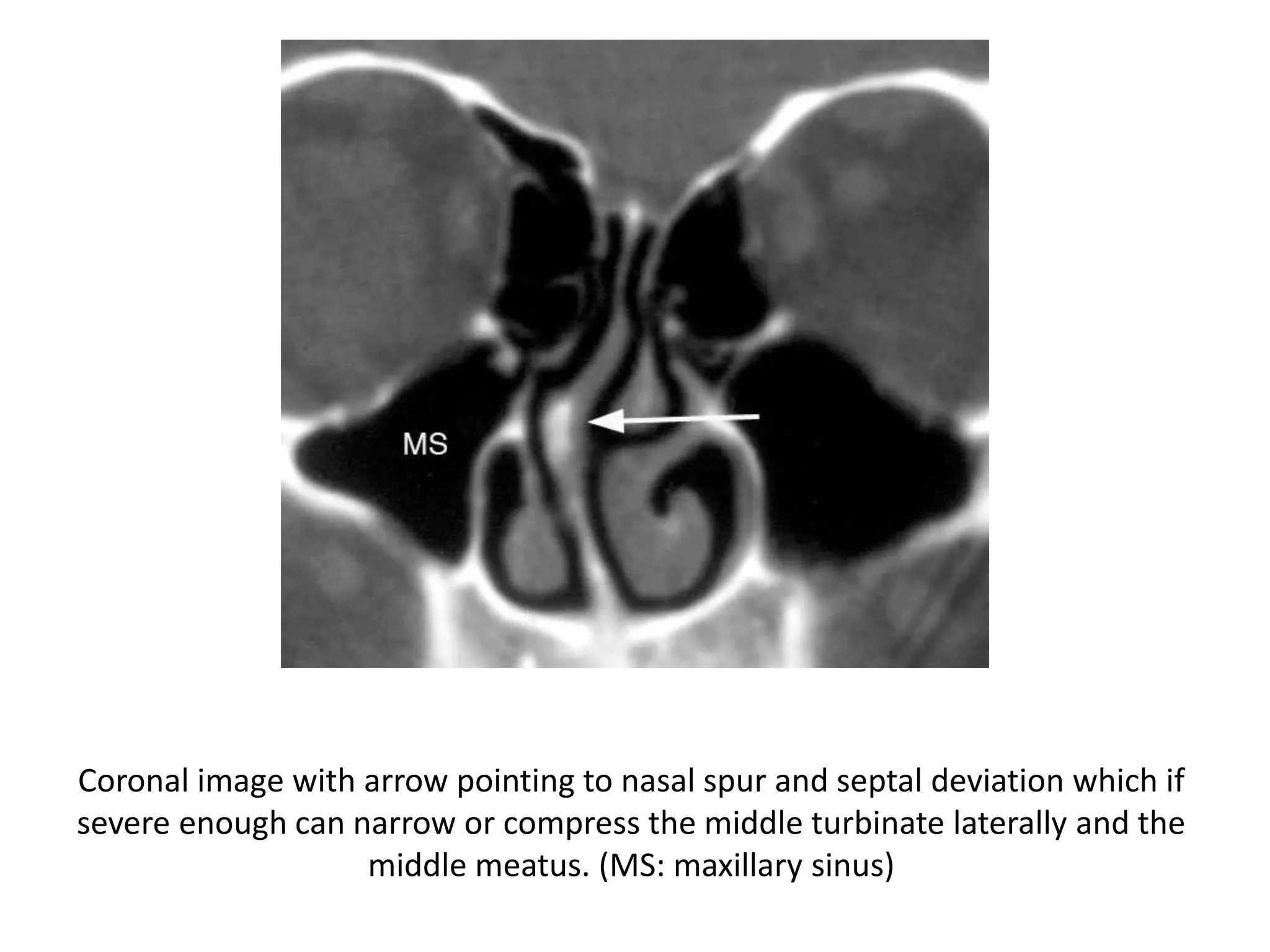
This document describes the anatomy and pathologies of the paranasal sinuses seen on CT imaging. It discusses the normal anatomy of the frontal and maxillary sinuses including common anatomic variants. Common inflammatory diseases are described such as acute sinusitis and its sequelae including mucus retention cysts, mucoceles, and intracranial extension. Other pathologies mentioned include osteomas.