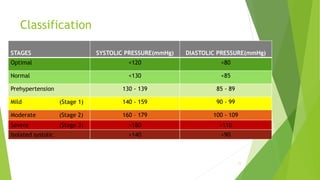
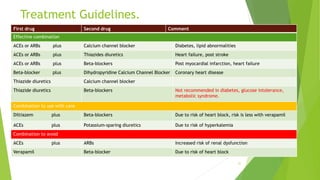
This document provides information on hypertension including its definition, etiology, signs and symptoms, classification, treatment and treatment guidelines. It defines hypertension as a condition where blood pressure is chronically elevated above 140/90 mmHg. The causes of hypertension are categorized as primary (essential) or secondary. Treatment involves non-pharmacological methods as well as various classes of antihypertensive drugs like ACE inhibitors, ARBs, calcium channel blockers, beta blockers, diuretics and vasodilators. The guidelines recommend starting treatment with one drug and adding a second from a different class if target is not reached after 3 months. Drug combinations should be used carefully due to risk of interactions.





































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














