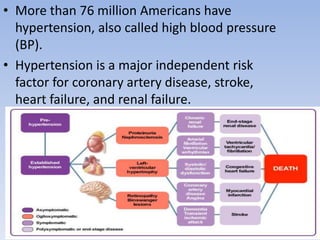
Hypertension, or high blood pressure, is defined as persistent elevated arterial blood pressure, affecting over 76 million Americans and approximately 970 million people worldwide. The majority have primary hypertension with no known cause, while secondary hypertension is linked to specific medical conditions. Treatment includes lifestyle changes and medications to lower blood pressure and prevent cardiovascular events.