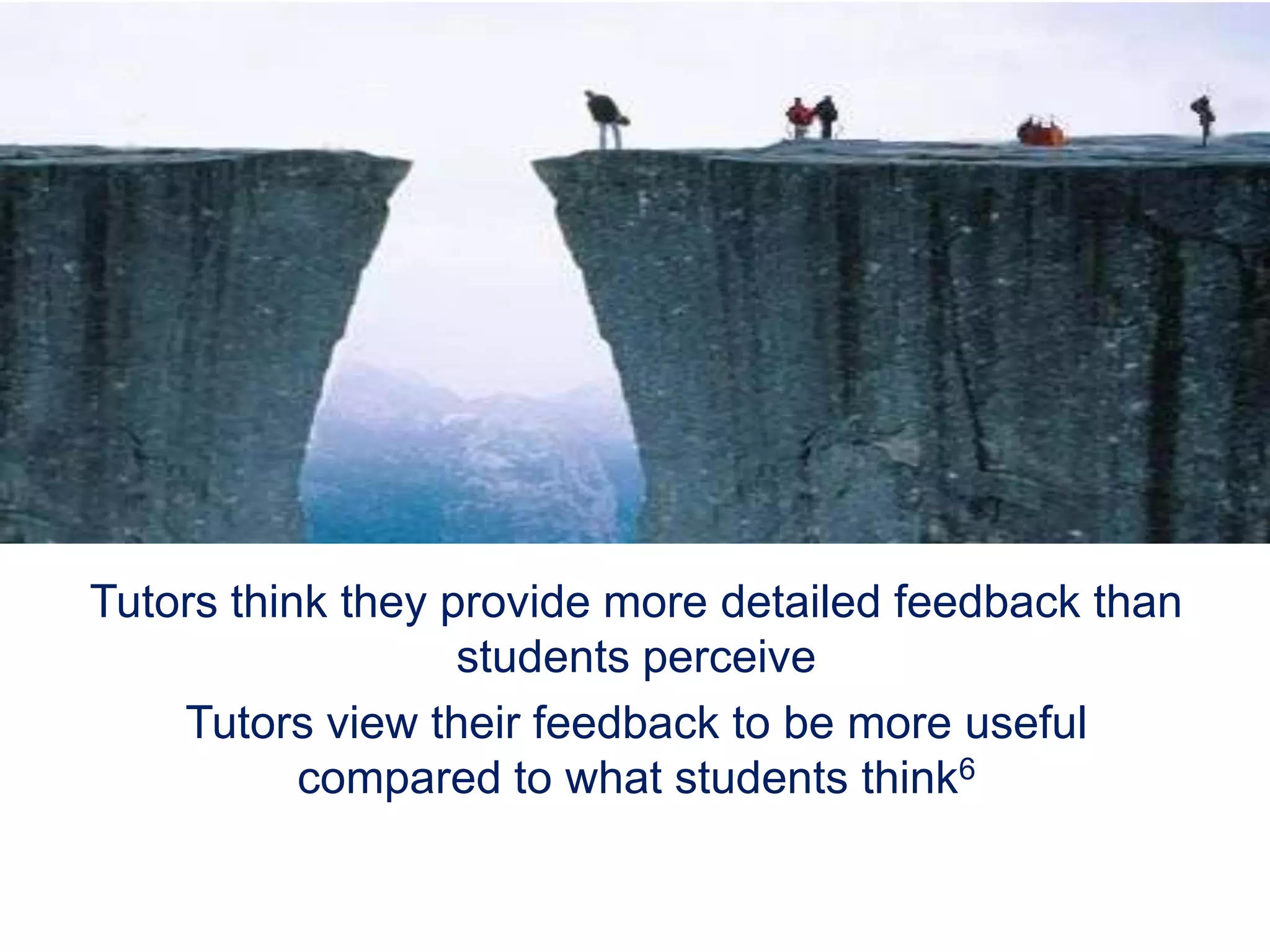
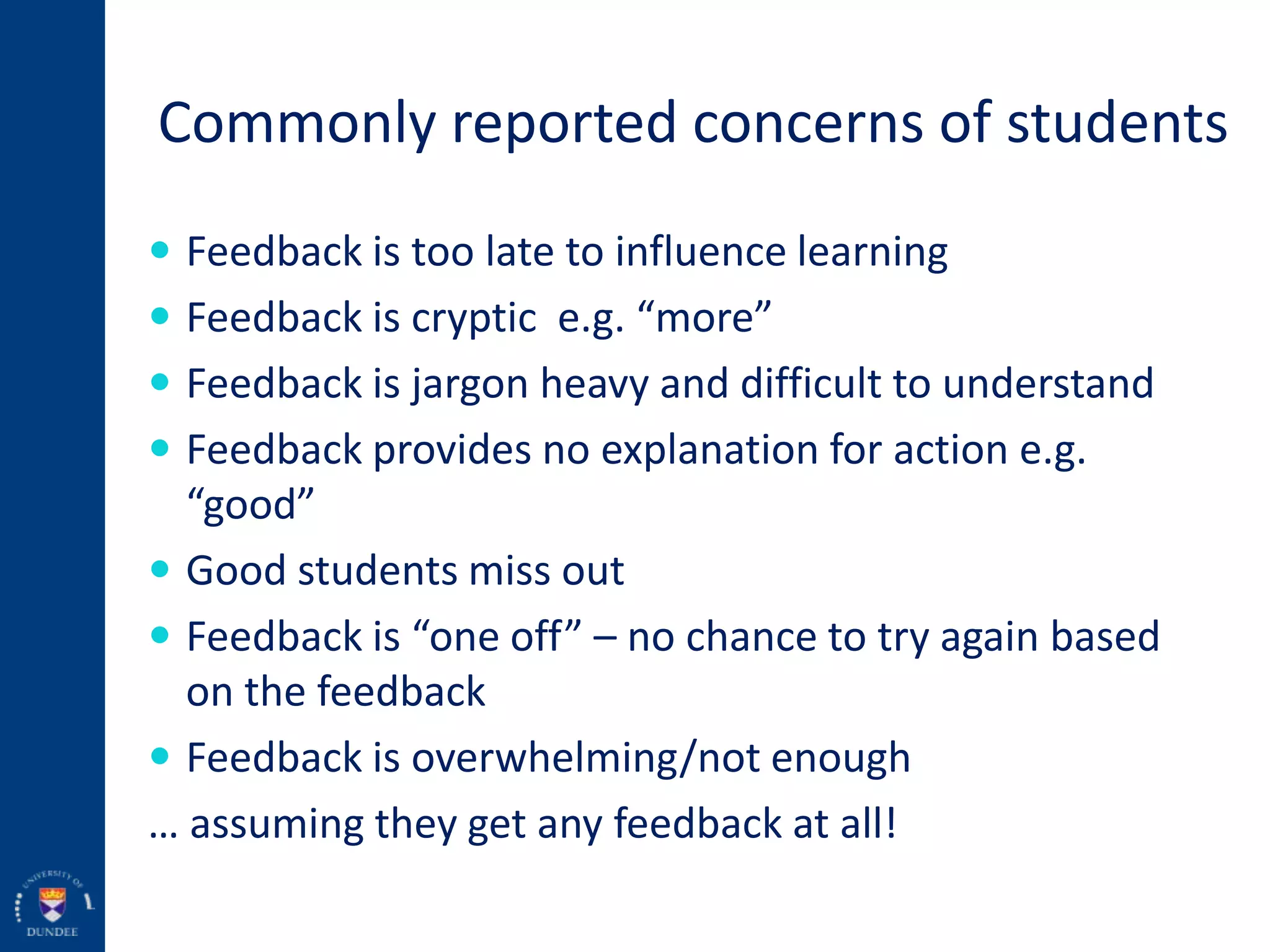
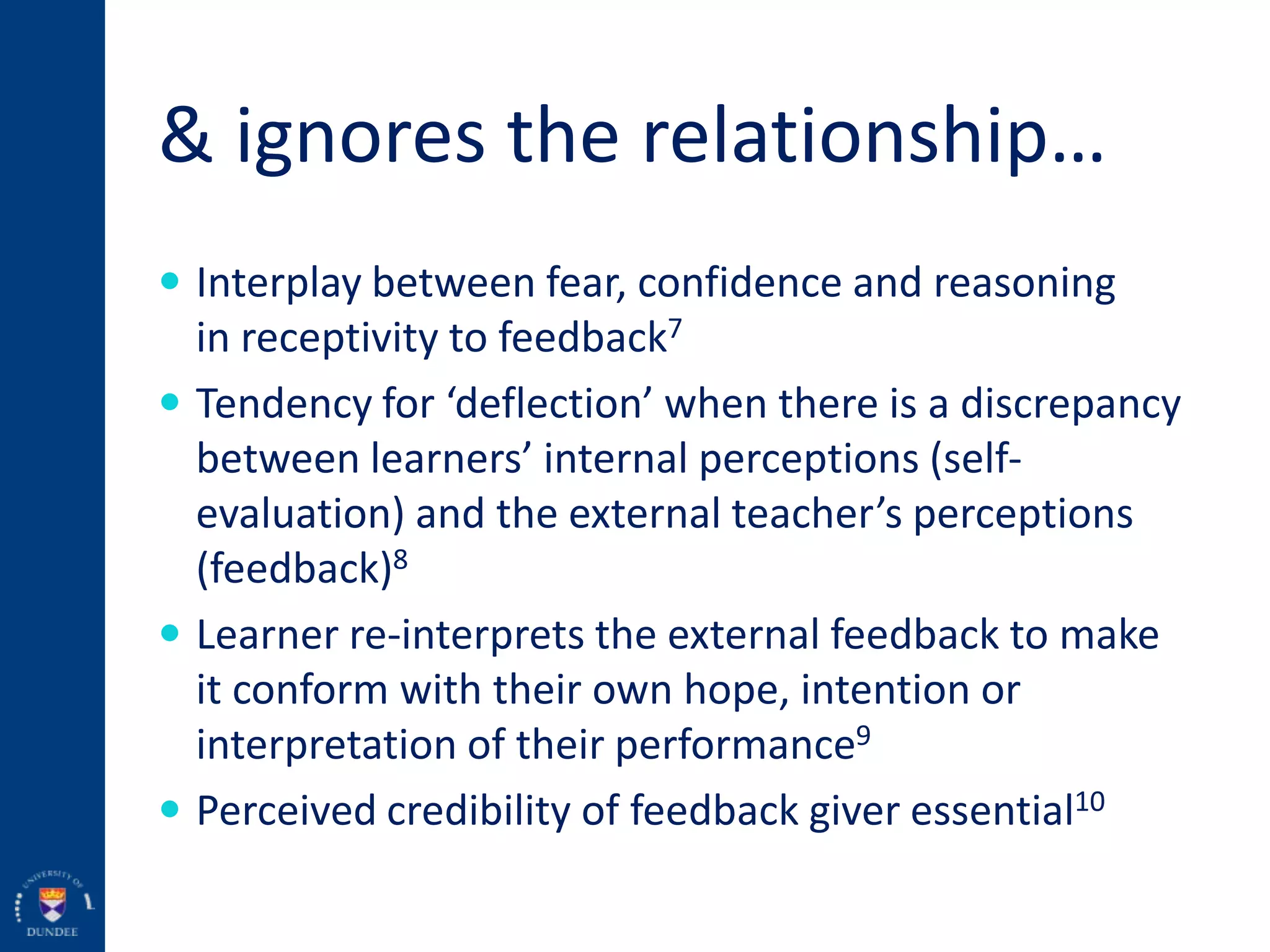
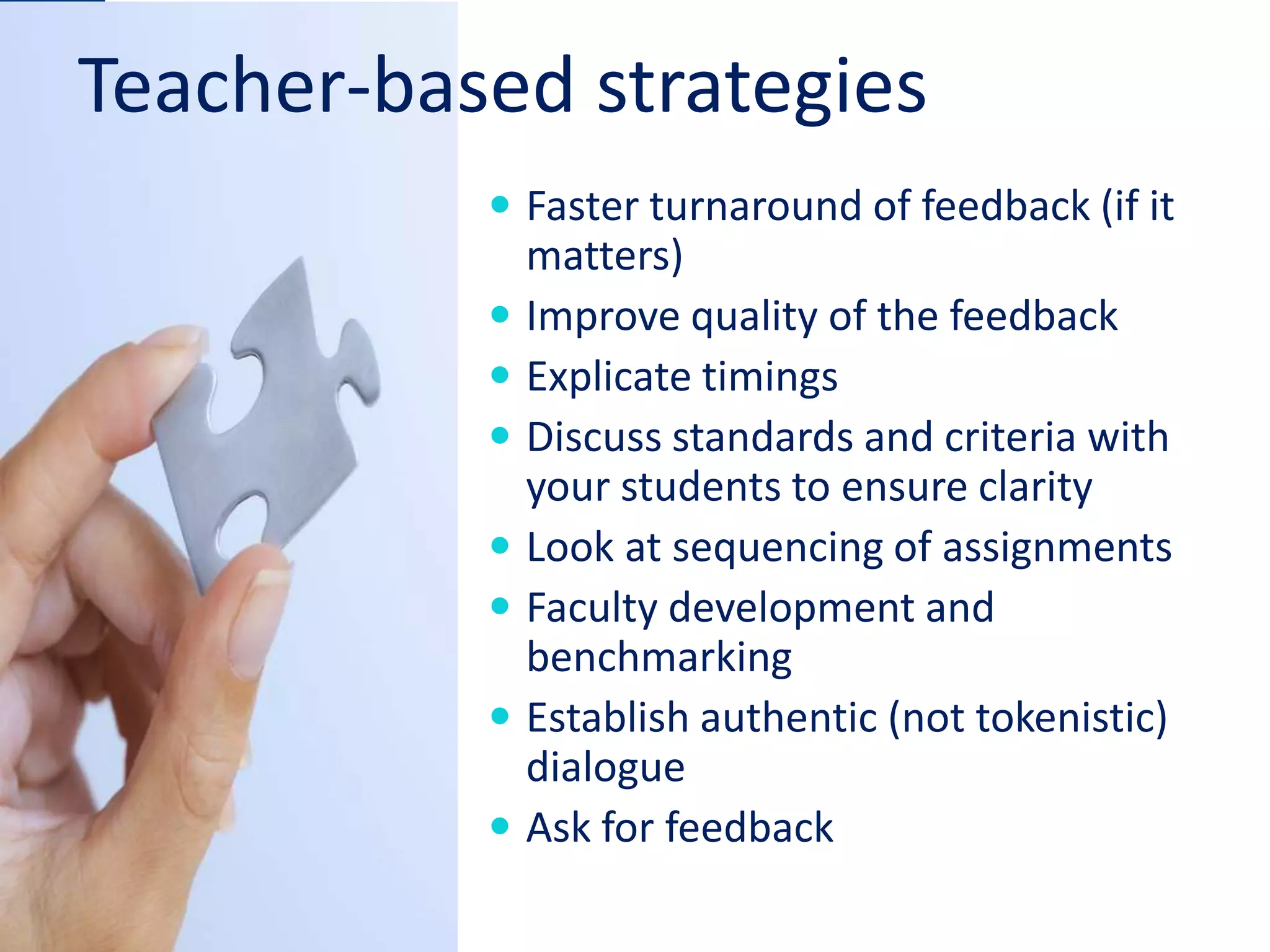
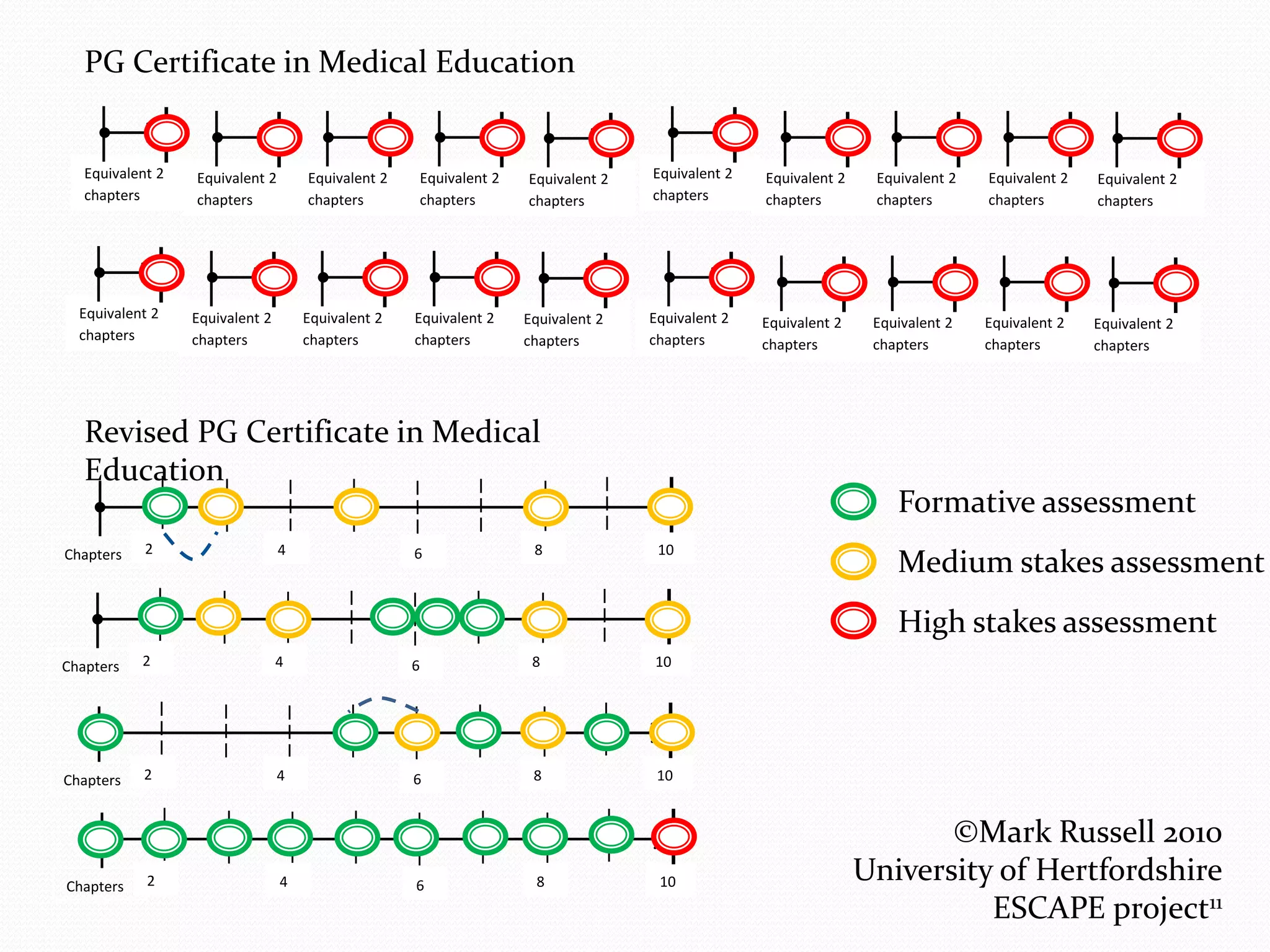
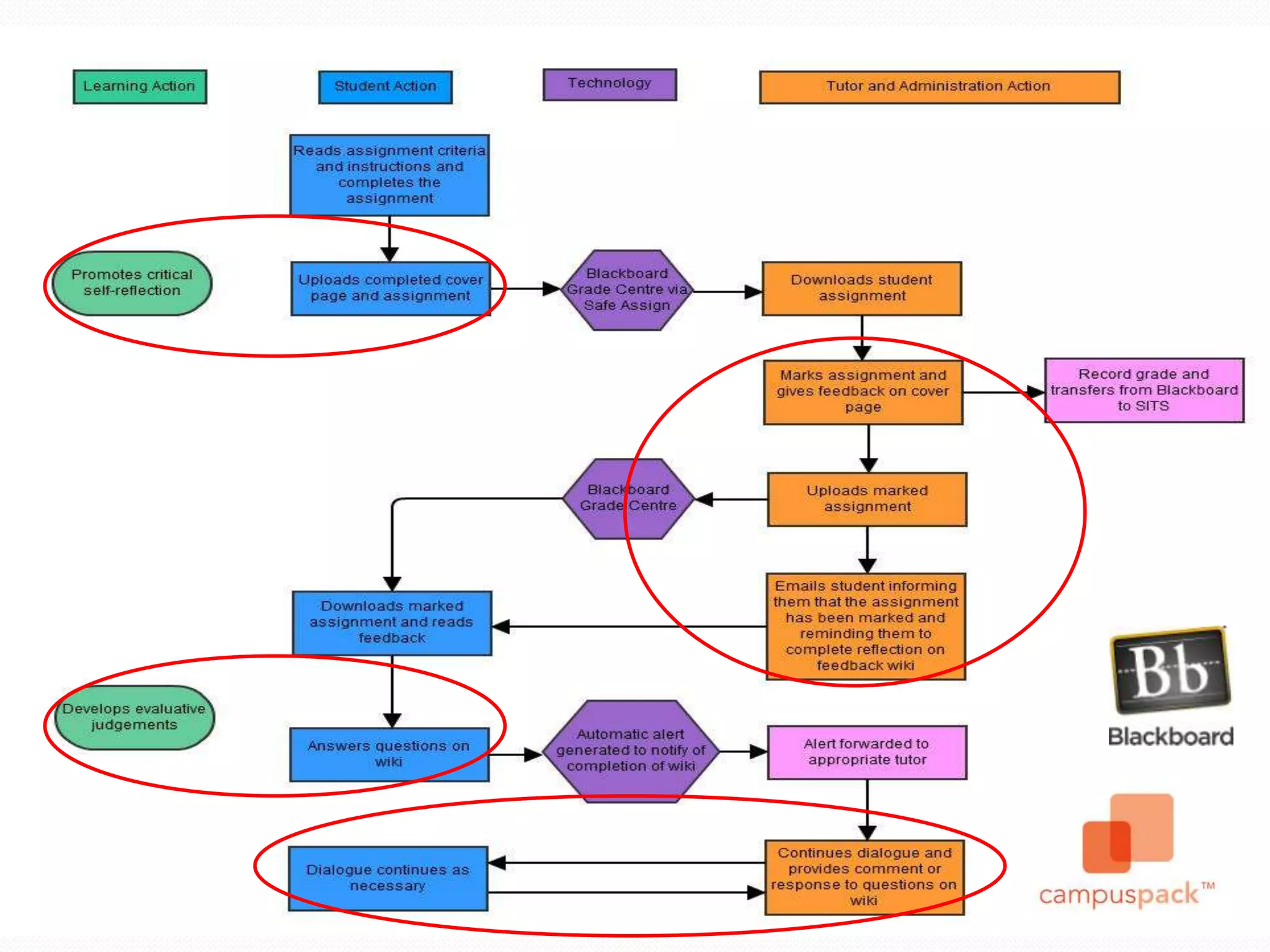
This document discusses feedback in medical education assessment. It begins by defining formative and summative assessment and explaining that feedback is valuable for both. Feedback is defined as information comparing a trainee's performance to a standard in order to improve. While feedback is seen as important, there is often a "feedback gap" where educators feel they provide more feedback than students perceive receiving. This gap can be bridged through actively involving students in feedback dialogues, with self-review, peer-review and discussion of standards. Both teacher and learner strategies are needed to improve the feedback process.