Download to read offline

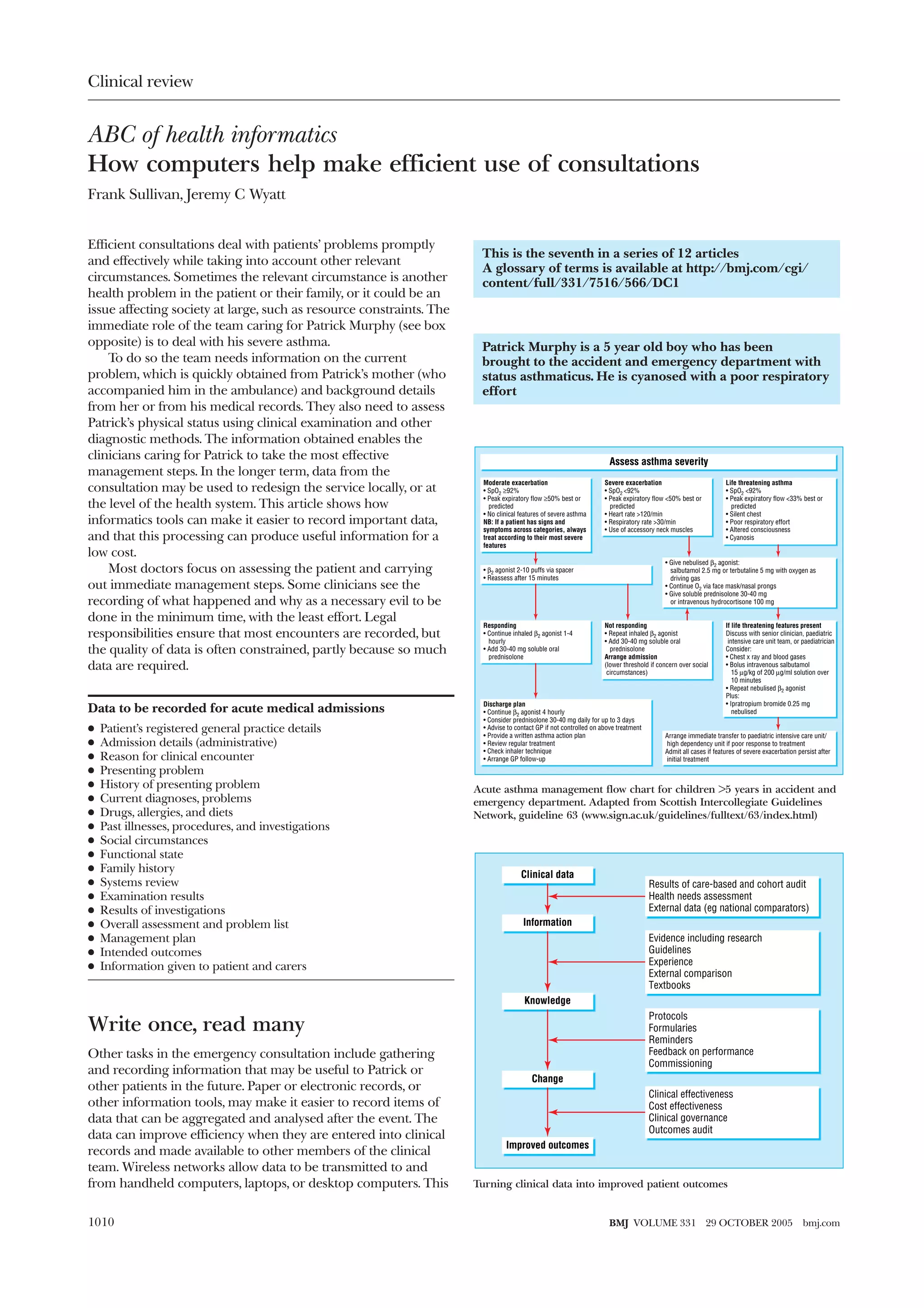



This document summarizes an article about how clinical informatics tools can help make patient consultations more efficient. It provides guidelines for assessing the severity of asthma exacerbations in children and outlines the steps for acute asthma management in an emergency department. Recording clinical data from patient encounters enables clinicians to better understand local service needs, compare performance to other health systems, and continuously improve care over time.





































![Asthma 2010 new gina guidelines[pediatric]](https://cdn.slidesharecdn.com/ss_thumbnails/asthma2010newginaguidelines-120921010443-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)













































