Downloaded 52 times




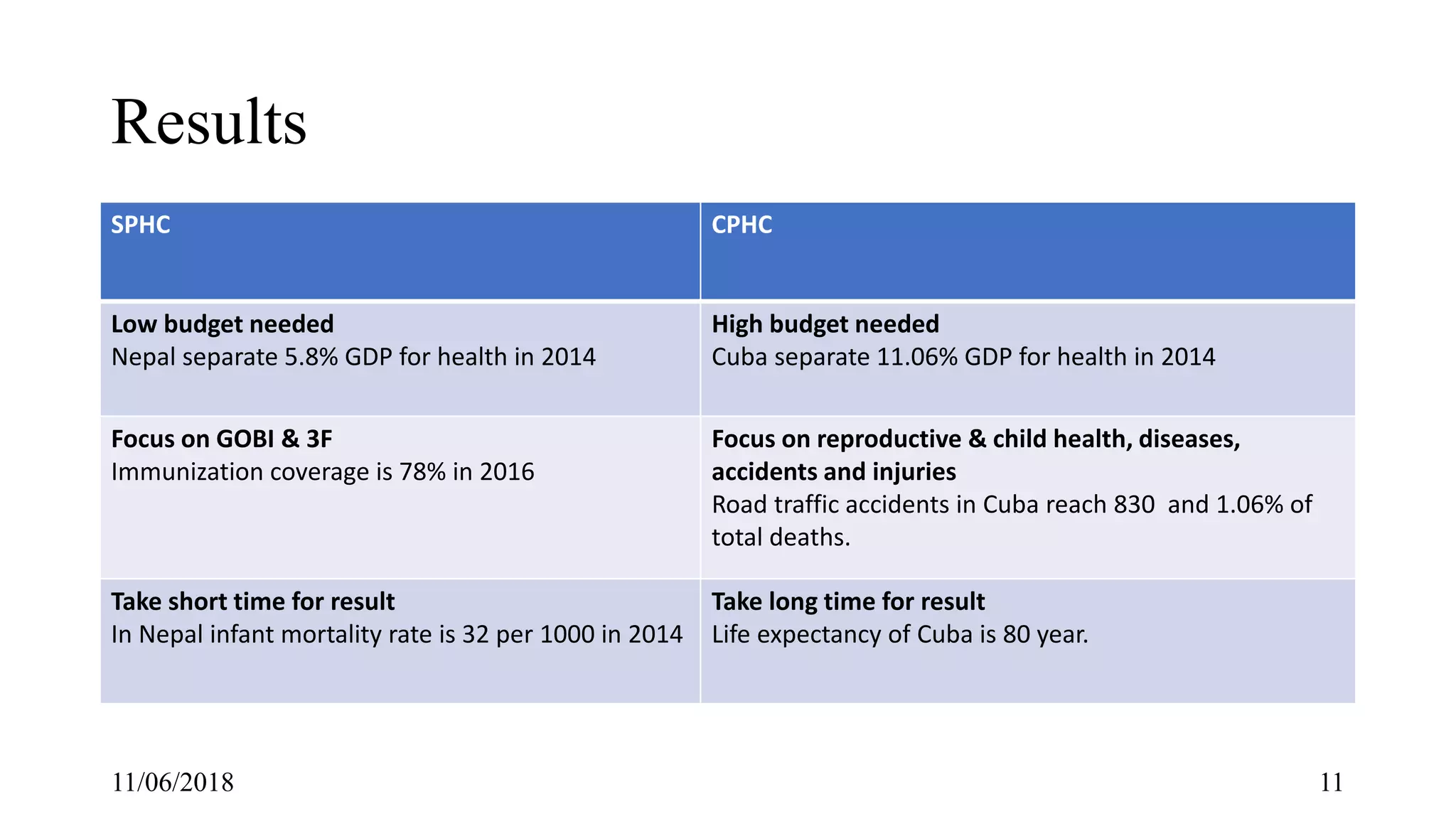







The document discusses selective primary health care (SPHC) versus comprehensive primary health care (CPHC). SPHC focuses on specific interventions like immunizations, while CPHC aims to improve overall population health through multisectoral coordination. Nepal has achieved success with SPHC but still struggles with CPHC indicators. While SPHC can reduce disease burdens quickly, CPHC is needed long-term to increase life expectancy. The recommendation is that Nepal should continue SPHC while gradually implementing more CPHC through improved coordination.