The document discusses challenges deaf and hard of hearing individuals face in accessing health care. It notes that deaf individuals often have difficulty communicating with providers due to lack of interpreters and reliance on notes or lip reading. This can lead to problems receiving diagnoses or explanations of health issues. A literature review found deaf people feel excluded from standard health resources and information. The research team conducted a survey that found most deaf respondents had trouble communicating with providers and did not have regular interpreter access. Many also experienced misdiagnoses or other health issues as a result of communication barriers.
Research Presentation on the Influence of Irrational Health Beliefs on Dental...Munir Gomaa
This research is conducted by Munir Gomaa in his third and fourth years of dental school and is titled "Influence of Irrational Health Beliefs in Adults on Dental-Related Perceptions, Practices, and Diseases in Adult and Pediatric Patients." The research examines how, as an example, irrational fears related to going to a dentist might contribute to that patient's overall oral health.
A presentation designed to inform health care workers about the components and importance of advance directives, with specific information for Massachusetts residents.
The issue of medical aliteracy has drawn both scholars and medical practitioners’ attention in the recent years. The negative cost of medical aliteracy has continued to constitute major threats to health related issue which has resulted in high mortality rate, high medical expenditure and medical underperformance among others. On this premise the study examined the influence of medical aliteracy among senior medical personnel. The study employed descriptive research design and Chi-Square to test the research hypotheses. A total number of 50 questionnaires were designed to collect information from the sampled population through a random sampling. From the result of the analysis it was revealed that factors such as ineffective supervision of medical personnel, low patient literacy level, lack of personnel-patients engagement could lead to medical aliteracy among senior medical personnel. Senior medical personnel have the knowledge of medical aliteracy and its implications on for medical personnel and the public. Medical aliteracy has an implication on health sector performance which includes increase in mortality rate, increase health expenditure, widening of the gap between patients – medical personnel communication among others. Perception of medical aliteracy has significant influence on medical personnel performance. The study concluded that, medical aliteracy is prevalent among medical personnel and patients and is associated with many poor medical outcomes in the health sector. It was however recommended that medical literacy training, schemes and programmes should be designed according to the needs of the different medical personnel and should therefore be included in medical professional training programs.
UCPMP guidelines pharma marketing code by http://www.dailyrounds.org/blog/ucp...Siddhartha Dash
Uniform code for pharmaceutical marketing Practices UCPMP Guidelines, Codes and Impact on Industry by DailyRounds.org (Largest network of doctors 200000+ & counting).
http://www.dailyrounds.org/blog/ucpmp-uniform-code-of-pharmaceuticals-marketing/
MCI Issues Public Notice on Ethics for Indian DoctorsAnup Soans
The Medical Council of India has issued a public notice in today's (19 August 2014) Hindustan Times:
"This is for the information of the public at large - Public is hereby informed that whenever they come across any unethical act or medical misconduct (commission/cuts, unnecessary investigation and nexus with drug companies, they should immediately approach and lodge a complaint with the MCI where the Medical Practitioner is registered.
Research Presentation on the Influence of Irrational Health Beliefs on Dental...Munir Gomaa
This research is conducted by Munir Gomaa in his third and fourth years of dental school and is titled "Influence of Irrational Health Beliefs in Adults on Dental-Related Perceptions, Practices, and Diseases in Adult and Pediatric Patients." The research examines how, as an example, irrational fears related to going to a dentist might contribute to that patient's overall oral health.
A presentation designed to inform health care workers about the components and importance of advance directives, with specific information for Massachusetts residents.
The issue of medical aliteracy has drawn both scholars and medical practitioners’ attention in the recent years. The negative cost of medical aliteracy has continued to constitute major threats to health related issue which has resulted in high mortality rate, high medical expenditure and medical underperformance among others. On this premise the study examined the influence of medical aliteracy among senior medical personnel. The study employed descriptive research design and Chi-Square to test the research hypotheses. A total number of 50 questionnaires were designed to collect information from the sampled population through a random sampling. From the result of the analysis it was revealed that factors such as ineffective supervision of medical personnel, low patient literacy level, lack of personnel-patients engagement could lead to medical aliteracy among senior medical personnel. Senior medical personnel have the knowledge of medical aliteracy and its implications on for medical personnel and the public. Medical aliteracy has an implication on health sector performance which includes increase in mortality rate, increase health expenditure, widening of the gap between patients – medical personnel communication among others. Perception of medical aliteracy has significant influence on medical personnel performance. The study concluded that, medical aliteracy is prevalent among medical personnel and patients and is associated with many poor medical outcomes in the health sector. It was however recommended that medical literacy training, schemes and programmes should be designed according to the needs of the different medical personnel and should therefore be included in medical professional training programs.
UCPMP guidelines pharma marketing code by http://www.dailyrounds.org/blog/ucp...Siddhartha Dash
Uniform code for pharmaceutical marketing Practices UCPMP Guidelines, Codes and Impact on Industry by DailyRounds.org (Largest network of doctors 200000+ & counting).
http://www.dailyrounds.org/blog/ucpmp-uniform-code-of-pharmaceuticals-marketing/
MCI Issues Public Notice on Ethics for Indian DoctorsAnup Soans
The Medical Council of India has issued a public notice in today's (19 August 2014) Hindustan Times:
"This is for the information of the public at large - Public is hereby informed that whenever they come across any unethical act or medical misconduct (commission/cuts, unnecessary investigation and nexus with drug companies, they should immediately approach and lodge a complaint with the MCI where the Medical Practitioner is registered.
Patients and their families are given a multitude of information about their health and commonly must make important decisions from these facts. Obstacles that prevent easy delivery of health care information include literacy, culture, language, and physiological barriers. It is up to the nurse to assess and evaluate the patient's learning needs and readiness to learn because everyone learns differently.
Before I begin I would like to say thank you for this study, althougcameroncourtney45
Before I begin I would like to say thank you for this study, although I am aware of the challenges that undocumented immigrants face, this article brings to light a whole different aspect of difficulties I did not consider. I am ashamed to admit that I have never thought about it from this perspective, much learned here.
The relationship between fear and its affect on health is very apparent as outlined in this study. Although fear can do many things, to include being a motivator, in the case of undocumented immigrants identified in this study it is paralyzing and results in higher levels of stress. Stress in turn results in significant and cumulative influences on health and health disparities (Reference study here). The three main sources of fear and how it relates to health are:
Cost:
The population identified in this study, due in large part to being undocumented, had a high rate of poverty, lower educational level, and high levels of transience. As expected this equates to an income level the precludes having health insurance in most cases. Fear experienced by these individuals was rooted not only in the cost that would be incurred from medical care, participants in the study also feared being identified by INS while being hunted down by bill collectors. Adding to the stress of healthcare cost, individuals were forced to choose between paying bills and buying food over paying for healthcare. Sadly, participants in this study looked at their diabetes and knew it would eventually kill them, just not today.
Language Barriers, Discrimination, and Immigration Status:
Participants in this study felt they were being discriminated against because many could not speak English, some recalled clinic/ER staff blatantly calling out and berating the participants for not speaking English and being in the country illegally. I find this particularly disgusting based on morality alone, medical professionals are charged with providing care to the needy, sick, and injured regardless of who they are. To further the participants stress level, communicating with physicians was difficult and often scary. Participants spoke of being made to feel guilty for needing an interpreter, and when they did have an interpreter, critical parts of the conversation were incorrect potentially causing serious medical issues with the patient.
Cultural Disconnect:
Participants described having difficulty speaking with medical staff about traditional remedies for the treatment of medical problems, some of the remedies (not all) were very effective in managing health issues with little side effects to the participants, including diabetes. Some individuals were embarrassed about what they had paid for the traditional medicine and that it ended up not working. Cultural disconnect made the participants fearful of what the provider might say about traditional remedies, negative feedback from the provider could potentially “spoil the normal identity of the patient” regarding ...
Rosemary Frasso's presentation from the
Penn Urban Doctoral Symposium
May 13, 2011
Co-sponsored with Penn’s Urban Studies program, this symposium celebrates the work of graduating urban-focused doctoral candidates. Graduates present and discuss their dissertation findings. Luncheon attended by the students, their families and their committees follows.
Health literacy is the most important factor in getting the proper health information and health services. Health literacy significantly affects healthcare accessibility, availability, affordability and eventually cost. Health literacy makes it possible for the people to actively participate in the healthcare decision making process.
(1) citation reference 150 words CultureHmong CultureC.docxmadlynplamondon
(1) citation reference 150 words
Culture
Hmong Culture
Considerations
In beginning the interview, a consideration to remember is that eye contact is considered rude to Hmong People and that tone of voice and body language are very important; taking too loudly, placing too much emphasis on words, or talking excessively with hands and arm movements can result in noncompliance (Carteret, 2012). As this patient is young and assumed to be mainstream with Western culture, she will likely be understanding and forgiving of eye contact, tone, and body language but interactions with older family members will require care.
Gender of the nurse might play a role in some assessments, it is important to ask if a male nurse has permission to touch the abdomen or auscultate the lungs, heart, or abdomen. Questions pertaining to sex should be private and held with a nurse who is the same gender as the patient, it is of note that questions or examinations regarding sexual health can be misinterpreted as judgment of promiscuity, resulting in refusal, so sex must be addressed with much explanation and rationale without judgment (Carteret, 2012). As infection can be related to sex or sexual contact, this should be addressed with this patient.
The patient’s language preference for the interview is also important. The patient is a young adult and in college, however, her preference might be Hmong, or the language typically spoken at home. Another consideration is, does the patient want anyone else present for her interview/assessment? Hmong People have a family structure that is patriarchal, meaning, the father generally very involved in decision making and can, ultimately have the final say on a topic or treatment; the mother is caregiver and may wish to be present to help take care of the patient. Hmong Elders also play a large role in decision making, with a Grandfather that might want to talk directly with the doctor and make decisions over the wishes of the patient or patient’s father (Carteret, 2012).
Hmong Culture has roots in animism, which is the belief that objects, places, animals, people, etc. all have spirits and bodies that maintain a natural balance (Duffy, J., Harmon, R., Ranard, D.A., Thao, B., & Yang, K. (2004). The fever in this patient could be related to an imbalance in her spirit, an inhabitation by another sprit that is making her ill, disapproval of recent behavior by dead ancestors, or a curse (Carteret, 2012). The family might elect to have a religious healer, or Shaman visit to perform holistic medicine on the patient, some of this medicine might cause burns or pinch marks with coining or skin pinching being common practices for illness (Khuu, Yee, & Zhou, 2017). An understanding of Western medicine might not be present, the patient or family may ask for dosages of antibiotics for infection or acetaminophen of fever to be increase or decrease based on how they feel; it is important to explain that medications are dosed on scientifi.
1. Health Care and the Challenges of Access for Deaf Persons in Erie County
Jenna Brick, Brittany Brown, Kennedy Lewandowski, and Amy Trabert
Social Work
The ability to access appropriate health care services is vitally important to the
physical and mental well-being of individuals (Sheppard, 2013). For the deaf
community, however, access to these critical services can be difficult. Deaf
individuals may lack opportunities to receive training to support a general
understanding of important health issues.
They often face challenges when communicating with health care providers due,
in part, to the lack of interpreters available in health care settings; heavy reliance
on written materials to facilitate understanding; and miscommunication related to
the technical nature of health information. Finally, those with particular needs
may be unable to secure specialized care because of challenges associated with
appropriate diagnosis.
Using survey data, the study team examined the unique health challenges among
local deaf individuals and discovered the barriers to health care assistance.
Recommendations for improvement are discussed as well.
Heiman, E., Haynes, S., & McKee, M. (2015). Research Paper: Sexual health
behaviors of Deaf American Sign Language (ASL) users. Disability And Health
Journal, 8579-585.
Heuttel, K., & Rothstein, W. (2001). HIV/AIDS knowledge and information sources
among deaf and hearing college students. American Annals Of The Deaf, 146(3),
280-286.
Jackson, M. (2011). Deafness and antenatal care: Understanding issues with access.
British Journal Of Midwifery, 19(5), 280-284.
Morere, D., Dean, P.M., & Mompremier, L. (2009). Mental health assessment of
deaf clients: Issues with interpreter use and assessment of person with diminished
capacity and psychiatric populations. Journal of the American Deafness &
Rehabilitation Association, 241-258.
O'Hearn, A. (2006). Deaf women's experiences and satisfaction with prenatal care: a
comparative study. Family Medicine, 38(10), 712-716.
Pereira, P., & Fortes, P. (2010). Communication and information barriers to health
assistance for deaf patients. American Annals Of The Deaf, 155(1), 31-37.
Sheppard, Kate. (2014). Deaf adults and health care: Giving voice to their stories.
Journal of the American Association of Nurse Practitioners, 26(9), 504-510.
doi:10.1002/2327-6924.12087
This research is based on preliminary findings with data still being collected.
Overall, there are barriers to accessing health care for deaf and hard of hearing
individuals mainly due to difficulty communicating with health care professionals.
The research team recommends that professionals in the health care setting receive
cultural competency and continuing education training on the deaf and hard of
hearing population. This training will help prevent problems with setting up
appointments, discussing symptoms, and encouraging health care providers to stop
relying on note taking and lip reading to share information. Ensuring access to
American Sign Language training for helping professionals is also imperative.
A review of the scholarly literature suggests that deaf and hard of hearing individuals often feel excluded
from resources that are generally available to hearing individuals in the larger society. This is
particularly true as it relates to health-related information, education, and services (Jackson, 2011).
Information about physical, mental, reproductive, and other health-related conditions is not always
readily accessible to deaf and hard of hearing individuals (Heuttel & Rothstein, 2001). In many cases,
information is distributed in paper form only and without the benefit of American Sign Language videos.
Similarly, health education is often difficult for deaf and hard of hearing individuals to secure because of
the lack of readily available interpretation assistance and limited offerings within the deaf community.
As a result, deaf and hard of hearing individuals may be unaware of the potential repercussions of certain
actions and/or may engage in behaviors that could put their health in jeopardy (Heiman, Haynes &
McKee, 2015).
Many deaf and hard of hearing individuals also face challenges when attempting to access health care
services. A common example is a deaf or hard of hearing individuals who has difficulty communicating
with office staff and may not hear his or her name when it is called for an appointment. This situation
can cause the individual to receive care well after their scheduled appointment, to miss their appointment
entirely, and/or to experience frustration (O’Hearn, 2006).
In addition to challenges communicating with office staff, deaf and hearing impaired individuals may
not be able to access professional interpreters during their appointment (Morere, Dean, Mompremier,
2009). Thus, many deaf or hard of hearing impaired individuals must rely on other methods to
communicate with health care professionals.
In some cases, deaf and hard of hearing individuals may be asked to have a family member or friend
assist with interpretation during the appointment. Many deaf or hard of hearing individuals
understandably are uncomfortable with fully disclosing their medical situation to friends or family
(Sheppard, 2014).
In the absence of an interpreter, a health care professional may attempt to communicate with a deaf or
hearing impaired individual via lip reading. This is highly problematic given the skill needed to be a
successful lip reader as well as the frequent use of medical terminology in the health care environment
(Pereira & Fortes, 2010). Similarly, health care professionals may resort to note writing – which is also
problematic given the use of jargon and the fact that note writing can also be very time consuming and
inaccurate.
Unfortunately, health care professionals may not have the time and/or patience to properly communicate
with deaf and hard of hearing individuals, leading to a lack of rapport, comfort, and trust between the
health care professional and their patient (Jackson, 2011). Challenges with communication can also
make it difficult for patients to fully disclose the nature and severity of their symptoms and could cause
them to be undiagnosed, underdiagnosed, or even misdiagnosed (Jackson, 2011; Morere, Dean &
Mompremier, 2009; O’Hearn, 2006).
ABSTRACT
LITERATURE REVIEW
METHODOLOGY
RESULTS
CONCLUSIONS
REFERENCES
HYPOTHESES
H1: Deaf and hard of hearing individuals experience difficulties communicating with health care
professionals about their health related to their deafness.
H2: Deaf and hard of hearing individuals do not secure regular access to an interpreter when
communicating with health care professionals about their health.
H3: Deaf and hard of hearing individuals experience health-related problems (including misdiagnosis,
being undiagnosed, or improperly diagnosed) because of difficulties communicating with their doctor.
H4: Deaf and hard of hearing individuals are not satisfied with their ability to easily access health-related
information and services.
DATA COLLECTION
The research team prepared a paper/web-based survey for use in data collection activities. Deaf and Hard
of Hearing individuals participating in meetings at Deaf Access Services (DAS) and the Buffalo Club of
the Deaf (BCD) (including sessions held in Niagara Falls and Jamestown, as well as the DAS employment
and BCD senior citizen groups) were asked to complete the survey with the help of an interpreter or
individually (availability or convenience sampling). In addition, individuals participating in the in-person
data collection were asked to provide information about the survey to friends, family members, and
acquaintances in order to increase the number of responses (snowball sampling). Each participant was
given the opportunity to be included in a raffle for one of five $25 gift cards as an incentive.
MEASUREMENT
To address each of the research team’s hypotheses, the following variables were included as part of data
collection:
Difficulties Communicating with Health Care Professionals: The survey included questions about
challenges respondents faced when communicating with health care professionals including difficulties
communicating with office staff, doctors, or nurses; reliance on notes or lip reading to share information;
lack of interpretation assistance; lack of explanation about health concerns; lack of relationship with health
care professionals; and misunderstanding about what is being communicated.
Professional Interpretation Assistance: Respondents were asked if they had regular access to an
interpreter when communicating with their doctor about their health.
Health-Related Problems: Respondents were asked if they ever experienced a health-related problem
(e.g., misdiagnosis, being undiagnosed, or improperly treated) because of difficulties communicating with a
health care professional.
Health-Related Information and Services: Respondents were asked if they were satisfied with their
ability to easily access health-related information and services related to their deafness/hearing impairment,
physical, mental, reproductive, sexual, and other health.
ETHICS AND DIVERSITY CONSIDERATION
Prior to the study, the research team received cultural competency training to ensure that members were
properly trained to work with deaf and hard of hearing individuals. The survey included information about
voluntary participation in the study including a clause stating that participants could refuse to answer any
question they were uncomfortable with or withdraw from the study at any time without fear of losing
access to resources. Privacy was ensured by asking questions specifically relevant to the study.
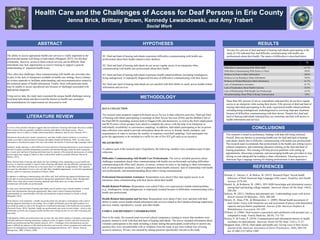
%
Difficulties Communicating With Office Staff 41.7%
Difficulties Communicating With Doctor or Nurse 50.0%
Reliance on Notes to Share Information 50.0%
Reliance on Lip Reading to Share Information 50.0%
Reliance on Printed Material to Share Information 41.7%
Lack of Interpretation Assistance 41.7%
Lack of Explanation About Health Concerns 25.0%
Lack of Relationships With Health Care Professional 16.7%
Misunderstanding About What Is Being Communicated 0.0%
Seventy five percent of deaf and hard of hearing individuals participating in the
study (n=18) indicated they had difficulty communicating with health care
professionals about their health. The nature of difficulties is described below.
More than fifty percent of survey respondents indicated they do not have regular
access to an interpreter when seeing their doctor. Fifty percent of deaf and hard of
hearing individual participating in the study experienced health related problems
including being misdiagnosed, underdiagnosed or receiving improper treatment
because of difficulties communicating with their doctor. Despite this, deaf and
hard of hearing individuals indicated they are somewhat satisfied with access to
health information and services.