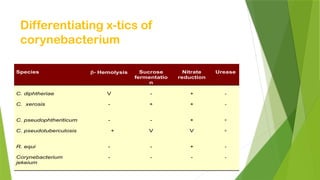
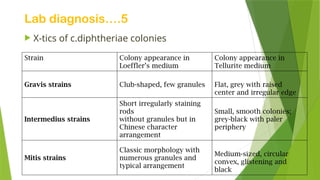
The document provides a detailed overview of gram-positive rods/bacilli, emphasizing the classification and characteristics of species such as Corynebacterium, Listeria, and Lactobacillus. It describes their pathogenicity, clinical features, laboratory diagnosis methods, as well as treatment and prevention strategies for infections like diphtheria and listeriosis. The information includes the biotyping of Corynebacterium diphtheriae, its toxin production, and relevant diagnostic tests for identifying these pathogens.












![2nd term lectures,_cd,_listeria,diphoids[1]](https://cdn.slidesharecdn.com/ss_thumbnails/2ndtermlecturescdlisteriadiphoids1-130109115805-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)









































