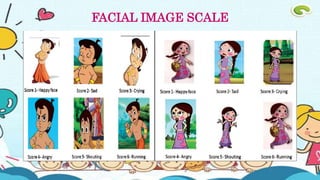
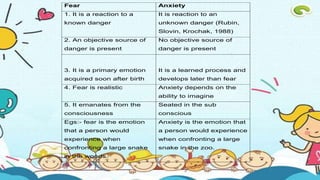
Fear and anxiety are defined as unpleasant emotions in response to threats. Fear is a response to realistic dangers while anxiety is a response to unknown dangers. Development of fears changes with age from unknown stimuli as infants to social fears as adolescents. Symptoms of fear include increased heart rate and tense muscles. Chronic fear can lead to issues like tiredness and avoidance. Assessment tools for dental fear include questionnaires and scales measuring facial expressions or selected points on an anxiety thermometer. Management of dental fear involves prevention strategies, behavioral treatments, and pharmacologic approaches depending on the level of fear.