3
Learning outcomes
• Atthe end of this module the students should be able
to:
• Identify gingival recession
• Categorize the different types of gingival recessions
• Manage patient with gingival recession
4.
4
Introduction
• Gingival recessionis the displacement of the gingival
soft tissue margin apical to the cemento-enamel
junction which results in exposure of the root surface
• The term “marginal recession” is considered to be
more accurate since the marginal tissue may have been
alveolar mucossa
5.
5
Cont’d
• Is acommon finding in many patients.
• The prevalence of gingival recession has been shown to
increase with age and can occur in patients with good
standards of oral hygiene as well as those with poor
oral hygiene and periodontal disease
6.
6
Etiology
• Direct mechanicalor physical influence on the gingival
tissues
or
• Indirectly due to an inflammatory reaction in the
gingival tissues
7.
7
Cont’d
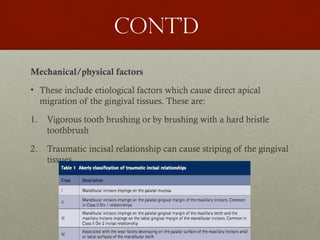
Mechanical/physical factors
• Theseinclude etiological factors which cause direct apical
migration of the gingival tissues. These are:
1. Vigorous tooth brushing or by brushing with a hard bristle
toothbrush
2. Traumatic incisal relationship can cause striping of the gingival
tissues
8.
8
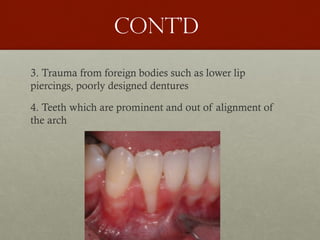
Cont’d
3. Trauma fromforeign bodies such as lower lip
piercings, poorly designed dentures
4. Teeth which are prominent and out of alignment of
the arch
9.
9
Cont’d
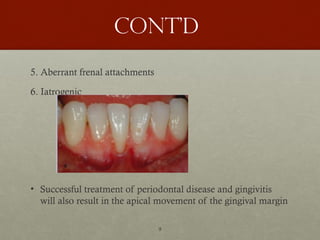
5. Aberrant frenalattachments
6. Iatrogenic
• Successful treatment of periodontal disease and gingivitis
will also result in the apical movement of the gingival margin
10.
10
Cont’d
Gingival recession causedby an inflammatory process
• There are various predisposing factors which can result
in recession due to inflammation of the gingival tissues
a. Gingival biotype: the thickness of the keratinized
tissue is an important prognostic factor
12
Cont’d
b. Periodontal disease
c.Poor marginal fit, inadequate crown emergence angles,
rough restoration surfaces and overhangs on restorations
d. Orthodontic tooth movement
13.
13
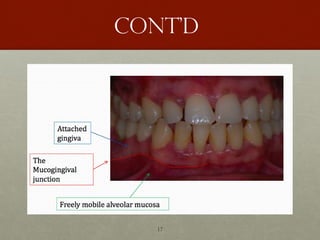
Measurement of
gingival recession
•Gingival recession is clinically measured from the CEJ
to the depth of the free gingival margins using
periodontal probs
14.
14
Gingival recession
classifications
• Sullivan& Atkins
1968
• Mlinek et al. (1973)
• Liu and Solt (1980)
• Bengue (1983)
• Miller (1985)
• Smith (1990)
• Nordland and
Tarnow (1998)
• Mahajan (2010)
• Cairo et. al. (2011)
• Rotundo et al. (2011)
• Ashish Kumar and
Masamatti (2013)
• Prashant et al. (2014)
15.
15
Sullivan & Atkins1968
• The bases for the classification was the depth and
width of the defect
• The four categories were
• Deep wide
• Shallow wide
• Deep narrow
• Shallow narrow
16.
16
Miller’s classification
• Dividedgingival recession defects into 4 categories
• Evaluates both soft and hard tissue loss
• Determines the level of root coverage achievable with a
free gingival graft
• It was therefore diagnostic and prognostic
18
Cont’d
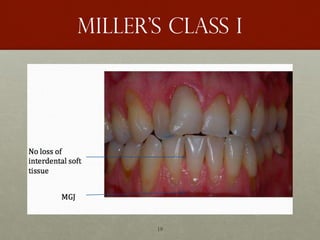
Class I
• Marginaltissue recession
which does not extend to the
mucogingival junction
(MGJ).
• There is no alveolar bone
loss or soft tissue loss in the
interdental area
• 100% root coverage
obtainable
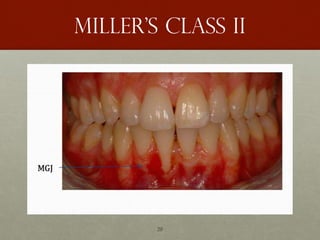
Class II
• Marginal tissue recession
which extends to or beyond
the MGJ
• There is no alveolar bone
loss or soft tissue loss in the
interdental area
• 100% root coverage
obtainable
21
Cont’d
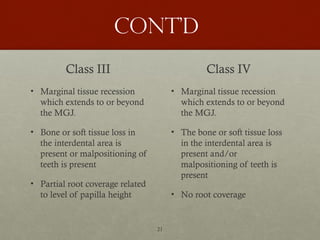
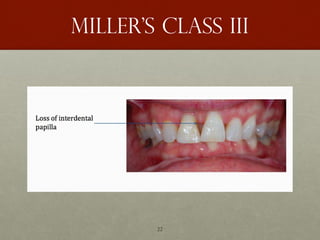
Class III
• Marginaltissue recession
which extends to or beyond
the MGJ.
• Bone or soft tissue loss in
the interdental area is
present or malpositioning of
teeth is present
• Partial root coverage related
to level of papilla height
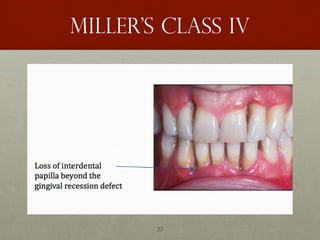
Class IV
• Marginal tissue recession
which extends to or beyond
the MGJ.
• The bone or soft tissue loss
in the interdental area is
present and/or
malpositioning of teeth is
present
• No root coverage
24
Limitations of miller’s
classification
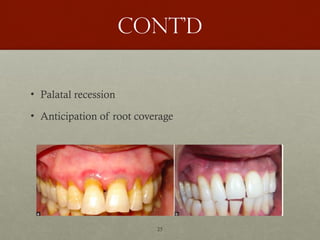
•Finding the MGJ
• Interdental bone/soft tissue loss is important point in
Cass III and IV. But the amount and type of bone loss
has not been specified
• Doesn't specify facial or lingual involvement of the
marginal tissue
• Recession of interdental papilla alone cannot be
classified
26
Nordland and Tarnow’s
Classification
•They developed a classification system for loss of
papillary height
• The system utilizes three identifiable landmarks: the
interdental contact point, the facial apical extent of the
CEJ, and the interproximal coronal extent of the CEJ
27.
27
Cont’d
• Normal: Interdentalpapilla fills embrasure space to the
apical extent of the interdental contact point/area.
• Class I: The tip of the interdental papilla lies between the
interdental contact point and the most coronal extent of
the interproximal CEJ
• Class II: The tip of the interdental papilla lies at or apical
to the interproximal CEJ but coronal to the apical extent
of the facial CEJ
• Class III: The tip of the papilla lies level with or apical to
the facial CEJ.
28.
28
Kumar and
Masamatti 2013
•This classification system is based on the
amalgamation of Miller’s classification with the certain
features of Nordland and Tarnow’s classification
• A distinct classification for gingival recession on the
palatal aspect is also introduced
29.
29
Cont’d
• This classificationcan be applied for facial surface of
maxillary teeth and facial and lingual surfaces of
mandibular teeth
• Interdental papilla recession can also be classified
according to this classification
30.
30
Cont’d
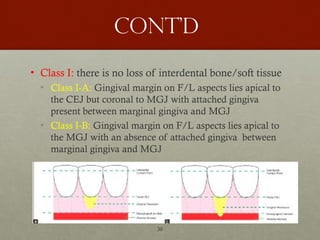
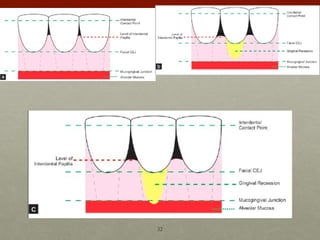
• Class I:there is no loss of interdental bone/soft tissue
• Class I-A: Gingival margin on F/L aspects lies apical to
the CEJ but coronal to MGJ with attached gingiva
present between marginal gingiva and MGJ
• Class I-B: Gingival margin on F/L aspects lies apical to
the MGJ with an absence of attached gingiva between
marginal gingiva and MGJ
31.
31
Cont’d
• Class II:the tip of the interdental papilla is located
between the interdental contact point and the level of
the CEJ mid-bucally/lingually
• Class II-A: there is no marginal tissue recession on F/L
aspect
• Class II-B: gingival margin on F/L aspect lies apical to
the CEJ but coronal to the MGJ with attached gingiva
present marginal gingiva and MGJ
• Class II-C: gingival margin on F/L aspect lies at or apical
to MJG with an absence of attached gingiva marginal
gingiva and MGJ
33
Cont’d
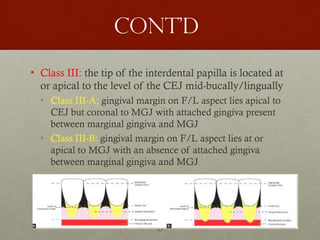
• Class III:the tip of the interdental papilla is located at
or apical to the level of the CEJ mid-bucally/lingually
• Class III-A: gingival margin on F/L aspect lies apical to
CEJ but coronal to MGJ with attached gingiva present
between marginal gingiva and MGJ
• Class III-B: gingival margin on F/L aspect lies at or
apical to MGJ with an absence of attached gingiva
between marginal gingiva and MGJ
34.
34
Proposed classification of
palatalGingival recession
• The position of interdental papilla remains the basis of
classifying gingival recession on the palatal aspect.
• The criteria of sub-classification has been modified to
compensate for the absence of MGJ
35.
35
Cont’d
• PR-I: dealswith marginal tissue recession on palatal
aspect with no loss of interdental bone or soft tissue
• PR-I-A: Marginal tissue recession ≤3mm from CEJ
• PR-I-B: Marginal tissue recession >3mm from CEJ
36.
36
Cont’d
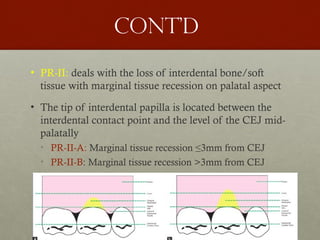
• PR-II: dealswith the loss of interdental bone/soft
tissue with marginal tissue recession on palatal aspect
• The tip of interdental papilla is located between the
interdental contact point and the level of the CEJ mid-
palatally
• PR-II-A: Marginal tissue recession ≤3mm from CEJ
• PR-II-B: Marginal tissue recession >3mm from CEJ
37.
37
Cont’d
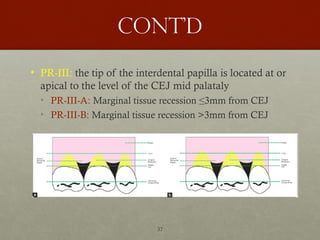
• PR-III: thetip of the interdental papilla is located at or
apical to the level of the CEJ mid palataly
• PR-III-A: Marginal tissue recession ≤3mm from CEJ
• PR-III-B: Marginal tissue recession >3mm from CEJ
41
Cairo classification
(2011)
• Basedon the assessment of CAL at both buccal and
interproximal sites
• Recession Type 1 (RT1): Gingival recession with no
loss of interproximal attachment. Interproximal CEJ
was clinically not detectable at both mesial and distal
aspects of the tooth
42.
42
Cont’d
• Recession Type2 (RT2): Gingival recession associated
with loss of interproximal attachment. The amount of
interproximal attachment loss (measured from the
interproximal CEJ to the depth of the interproximal
pocket) was less than or equal to the buccal attachment
loss (measured from the buccal CEJ to the depth of the
buccal pocket)
43.
43
Cont’d
• Recession Type3 (RT3): Gingival recession associated
with loss of interproximal attachment. The amount of
interproximal attachment loss (measured from the
interproximal CEJ to the depth of the pocket) was
higher than the buccal attachment loss (measured from
the buccal CEJ to the depth of the buccal pocket)
44.
44
Limitations of cairo
system
•Does not consider the remaining width of attached
gingiva
• Doesn’t consider relationship of gingival margin, and
MGJ, which play a very important role and govern the
choice of treatment procedure
• Doesn’t consider tooth malposition which greatly
affects the treatment outcome.
45.
45
Cont’d
• This classificationis a treatment oriented classification
‐
to forecast the potential for root coverage through the
assessment of interdental CAL. (Tonetti et al. 2014)
• In order to account for other factors associated with
the predictability of root coverage with the different
mucogingival surgical interventions, this classification
should be supplemented with other relevant diagnostic
elements (depth of the gingival recession, gingival
thickness, keratinized tissue width, presence of the
CEJ, associated cervical lesions).
46.
46
Cont’d
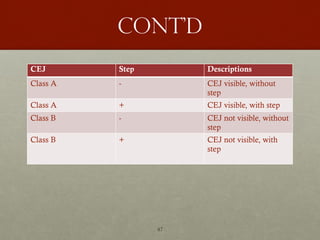
• The developmentof NCCLs occurs frequently on
exposed root surfaces and is associated with deeper
gingival recessions. These NCCLs are usually
accompanied by the loss of the CEJ and/or formation
of lesions on the tooth surface (loss of substance with
presence of a root surface concavity >0.5mm [step]).
• In the new 2017 classification (Cortellini & Bissada
2018) it is possible to identify four different clinical
situations which are shown on the following table:
47.
47
Cont’d
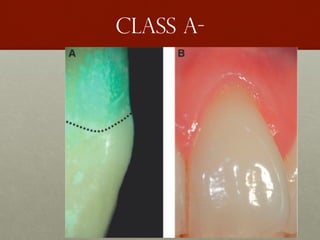
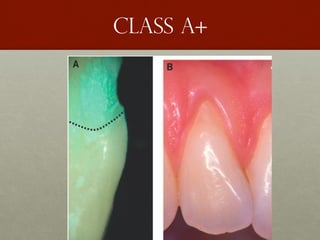
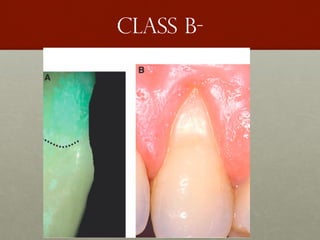
CEJ Step Descriptions
ClassA - CEJ visible, without
step
Class A + CEJ visible, with step
Class B - CEJ not visible, without
step
Class B + CEJ not visible, with
step
52
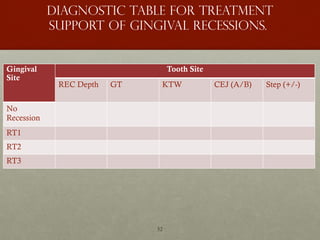
Diagnostic table fortreatment
support of gingival recessions.
Gingival
Site
Tooth Site
REC Depth GT KTW CEJ (A/B) Step (+/-)
No
Recession
RT1
RT2
RT3
53.
53
PATIENT
COMPLAINTS/CONCERNS
• Gingival recessionis a common feature seen in many
patients. Some patients will be unaware of the
condition, others will be aware of it but not concerned
about it whereas some will be concerned about it and
will want it corrected.
• Some of the concerns are
• Esthetics
• Sensitivity
54.
54
TREATMENT
NON-SURGICAL TREATMENT OPTIONS
1.Monitoring and prevention of further recession
• If the recession defect is minimal
• not in the aesthetic zone
• There is no associated dentine hypersensitivity or root
caries
• Manage the etiology and advise to keep their oral
hygiene
55.
55
Cont’d
2. Desensitising agents,varnishes and dentine bonding
agents to treat dentine hypersensitivity
• If the patient’s main complaint is sensitivity and
aesthetics are not a concern
• Patients suffering from dentine hypersensitivity may
avoid brushing areas which are sensitive
56.
56
Cont’d
3. Composite restorations
•Small localized recession defects with sensitivity, wear
or caries of the root surface can be corrected by
bonding tooth colored composite over the exposed root
surface
• In some cases using tooth colored composite in this
way may not be aesthetically acceptable and alternative
options would need to be considered to restore the
aesthetics
58
Cont’d
4. Pink porcelainor composite
• in some patients surgery may not be a viable option or
an option they wish to pursue
• With advances in bonding agents and the development
of pink ceramics and resin composite materials, it is
possible to use gingival colored porcelain or
composites over the root surface to eliminate dentine
hypersensitivity
59.
59
Cont’d
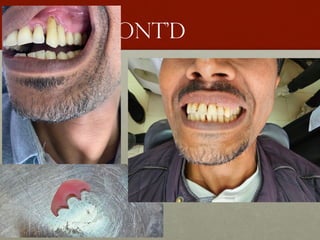
5. Removable gingivalveneers
• Some patients will have multiple sites of recession in
the anterior aesthetic zone which is most commonly
associated with periodontal disease
• This results in exposed root surfaces and appearance of
spacing between the teeth where the dental papillae
have been lost, often referred to as ‘black triangles’.
62
Cont’d
6. Orthodontics
• Teethwhich may be malpositioned buccally/labially
through development may have a buccal dehiscence
and associated recession
• This can be corrected by means of orthodontics
therapy
64
Cont’d
Factor affecting outcomeof periodontal plastic surgery
• Patient-related factors:
• poor oral hygiene following the procedure will negatively
influence the success of root coverage procedures
(Caffesse et al. 1987).
• Predominant causative factor (abuse brushing)
• Smoking (Miller 1987, Trombelli & Scabbia 1997, Muller et al.
1998, Zucchelli et al. 2000),while other studies have shown no
differences between smokers and non-smokers (Tolmie et al.
1991, Harris 1994).
65.
65
Cont’d
• Site-related factors:
• level of interdental periodontal support
• Dimensions of the recession defect.
• Wennstrom & Zucchelli (1996) reported in a study comparing
the treatment effect of coronally advanced flap and free
connective tissue graft procedures that complete root coverage was
observed in only 50% of the defects with an initial depth of 5
mm and wide ‘more than 3mm’ compared to 96% in shallow
and narrow defects ‘less than 3mm’.
66.
66
Cont’d
• Technique-related factors:
•flap thickness :Complete root coverage at sites with Miller
Class I-II recessions was obtained only when the flap
thickness was 0.8 mm. However, whether a full or split
thickness pedicle graft is used for root coverage was not
found to influence the treatment outcome ( Espinel &
Caffesse 1981)
• Flap tension :reported to be an important factor for the
outcome of the coronally advanced flap procedure(Allen
& Miller 1989
67.
67
Cont’d
• The connectivetissue areas lateral to the recession defect
• Although it may be considered important for the retention of the
advanced flap when positioned over the root surface, the
dimension of the interdental papilla is not a prognostic factor for
the clinical outcome of the procedure (Saletta et al. 2001)
• The thickness of the graft :With regard to free graft procedures,
the thickness of the graft is a factor influencing the success of
treatment procedure (Borghetti & Gardella 1990). A thickness of
the free graft of about 2 mm is recommended.
68.
68
Free gingival graft
•Free grafts involve harvesting soft tissue from a distant
site in the mouth and grafting it over a localized
recession defect.
• The free gingival graft first described by Nabers,
involves harvesting epithelialized tissue from the palate
and placing it on a connective tissue bed at recipient
site with the aim of covering the exposed root surface
and/or increasing the width of keratinized tissue .
• Can be one stage or two-stage procedure to cover the
exposed root surface
69.
69
Cont’d
Indications
• Increasing theamount of keratinized tissue (more
specifically, attached gingiva)
• Increasing the vestibular depth
• Increasing the volume of gingival tissues in edentulous
spaces (preprosthetic procedures)
• Covering roots in areas of gingival recession
70.
70
Cont’d
Contraindications
• A perceptiblemismatch in color between the donor site
and the gingiva adjacent to the recipient site
• A lack of thick donor tissue; the recommended thickness
is a minimum of 1.5 mm
• A class III or class IV recession defect
• A root surface of excessive mesiodistal width coupled
with interproximal tissue that is too narrow to support
the blood supply
72
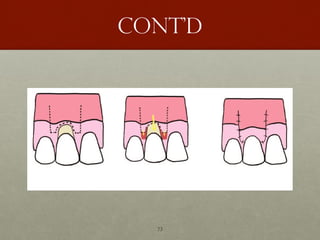
Coronally advanced
flap (caf)
•First describe by Bernimoulin et al.
• The amount of coronal advancement required is
determined by measuring the height of the recession
defect. The same length is then measured from the tip
of the papilla towards the apex and horizontal
incisions are placed through the tissue for a split
thickness flap. Vertical relieving incisions are placed at
the distal line angle of one tooth anteriorly and mesial
line angle of one tooth posterior to the tooth with the
recession defect
74
Cont’d
Requirement of CAF(Maynard 1977)
• The presence of shallow crevicular depths on proximal Surfaces
• Normal interproximal bone heights
• Tissue height within 1 mm of the cemento-enamel junction of
adjacent teeth
• Six-week healing of the free gingival graft prior to coronal
positioning
• Reduction in root prominence
• Adequate release of the flap during the second-stage surgery to
prevent retraction during healing
75.
75
Cont’d
One stage CAF
•Prerequisites
• Shallow marginal recession
• Minimum keratinized tissue width (3 mm)
• Periodontium not too thin
76.
76
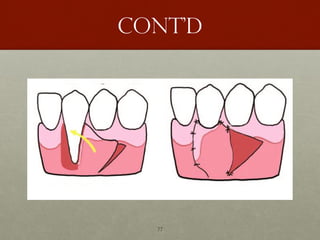
Pedicle flap
• Thepedicle flap was first described by Grupe and Warren as
a laterally repositioned full thickness flap. Here the donor
tissue is taken from one side of the recession defect and
repositioned over the exposed root surface.
• This was later modified by Hattler with the use of a split
thickness flap repositioned in a similar way to cover multiple
exposed root surfaces.
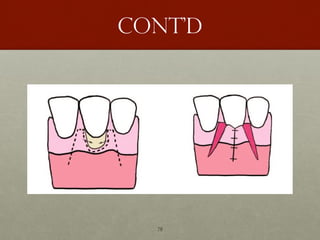
• Soon after, Cohen and Ross described the double-papilla
repositioned flap for use in areas where there was insufficient
keratinised gingival tissue on any one side of the recession
defect to reposition and cover the exposed root surface.
79
Cont’d
INDICATIONS
• Inadequate amountof attached gingiva
• Recession next to an edentulous area
PREREQUISITES
• Thick periodontal biotype
• Preferably deep vestibule
80.
80
Cont’d
Contraindications
• Insufficient adequatedonor tissue
• A shallow vestibule
• Presence of high frenum attachments
• Multiple adjacent recessions
• When recession will occur at the donor site as a result of the
procedure
81.
81
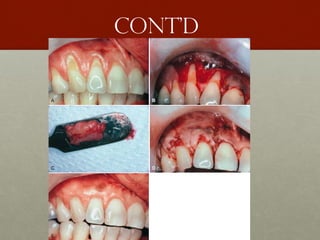
Sub-epithelial connective
tissue graft
•The subepithelial connective tissue (CT) graft was first
described by Raetzke with the use of an envelope
pedicle flap.
• Langer and Langer described an alternative technique
which involved placing the subepithelial connective
tissue graft with a coronally positioned pedicle flap for
covering exposed root surfaces
82.
82
Cont’d
Indications
• A lackof adequate donor tissue for a lateral sliding flap
• The presence of isolated wide recessions
• The presence of multiple root recessions and a minimal zone of
attached gingiva requiring augmentation
• The presence of recession adjacent to an edentulous area
requiring ridge augmentation
• The presence of recession in an area where esthetics is of great
concern
• McGuire showed that the technique can be used on previously
restored root surfaces
84
Coronally Repositioned Flapwith
Membrane or Emdogain or Alloderm
Indication
• Moderate to severe gingival recessions
• Thin palate , anatomical limitation of palate
• Patient reluctant to have a second surgery site
#7 Tooth brushing: mainly localized and seen in patients with good oral hygiene
#9 aberrant fraenal attachments have been mentioned as a cause of recession due to an apical pull on the gingival tissues, however, the evidence for this is poor




![46
Cont’d
• The development of NCCLs occurs frequently on
exposed root surfaces and is associated with deeper
gingival recessions. These NCCLs are usually
accompanied by the loss of the CEJ and/or formation
of lesions on the tooth surface (loss of substance with
presence of a root surface concavity >0.5mm [step]).
• In the new 2017 classification (Cortellini & Bissada
2018) it is possible to identify four different clinical
situations which are shown on the following table:](https://image.slidesharecdn.com/4-250329153926-0c5628e4/85/Gingival-recession-and-it-s-classification-46-320.jpg)