Download to read offline
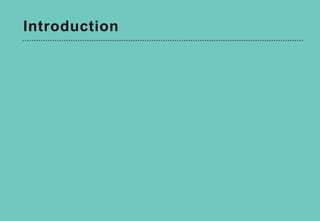
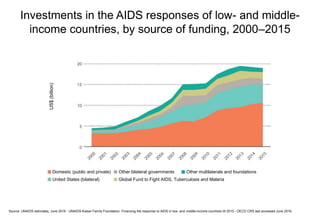
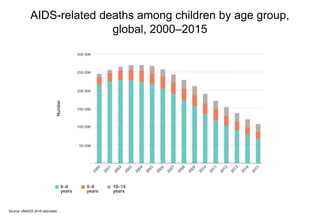
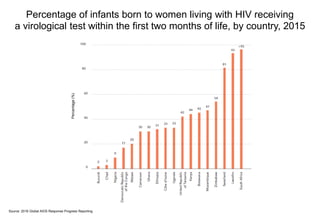
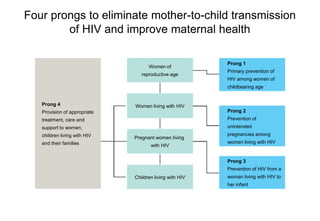
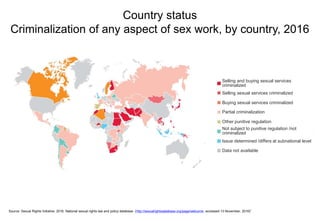
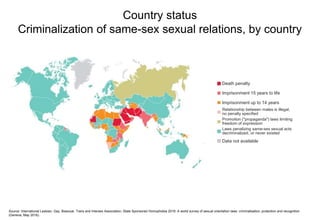
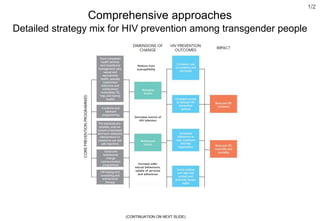
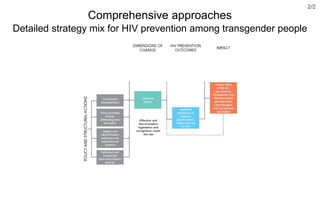
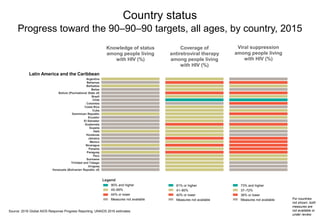
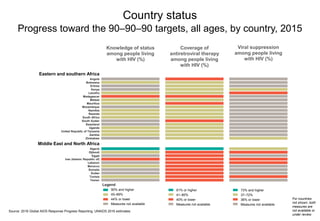
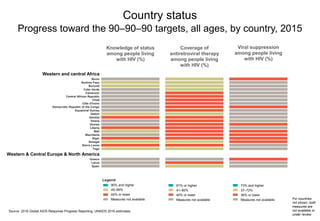
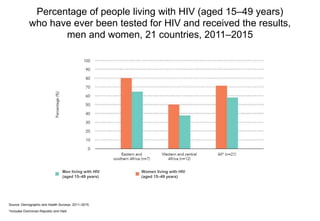


This document summarizes the life-cycle approach to addressing HIV. It discusses progress and challenges in preventing mother-to-child transmission of HIV and treating children living with HIV. It also examines new HIV infections and interventions among young people, key populations, and people at different stages of life. Charts and data from countries worldwide are presented on topics like HIV testing, condom use, treatment coverage, and criminalization status.









































![2014_HIV_prevention_and_control[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/2014hivpreventionandcontrol1-220810084127-bc7e0dd9-thumbnail.jpg?width=640&height=640&fit=bounds)













































