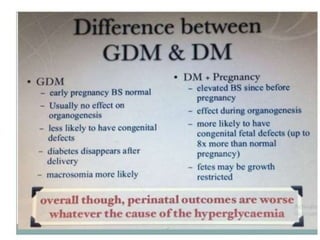
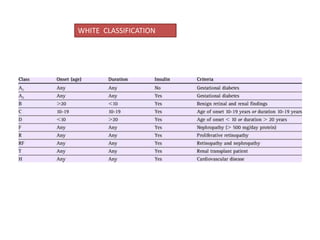
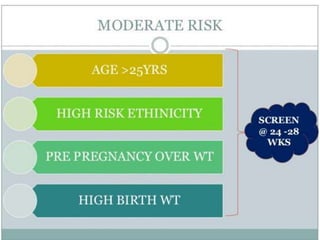
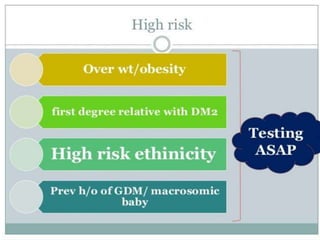
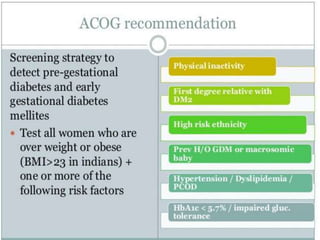
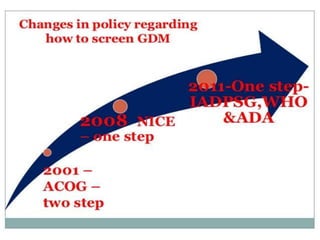
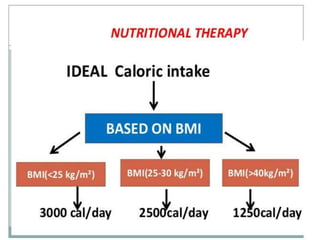
This document discusses gestational diabetes mellitus (GDM). It begins by defining GDM as glucose intolerance that begins during pregnancy. The prevalence of GDM is approximately 18% globally and is increasing due to lifestyle factors. The document then discusses the classification, epidemiology, pathophysiology, screening, and management of GDM. Key points include that GDM occurs in approximately 7% of pregnancies, is associated with increased insulin resistance during pregnancy, and screening and treatment can help reduce maternal and fetal complications. Management involves medical nutrition therapy, exercise, insulin therapy if needed, and monitoring during labor and delivery.