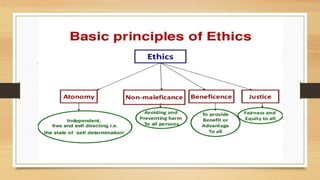
The document outlines the principles of medical ethics, including autonomy, beneficence, non-maleficence, and justice, and their historical evolution from the Hippocratic Oath to modern codes. It emphasizes informed consent, confidentiality, and the ethical challenges faced in patient care, particularly in complex decision-making situations. The document also highlights the importance of ethical frameworks in addressing dilemmas and improving healthcare outcomes.