This document summarizes a gender workshop for physicians that covered key concepts related to gender and health. It began with defining terms like sex, gender, gender identity and sexual orientation. It explained how gender impacts health through influences on recognition and management of illness as well as health policies. Specific examples showed how gender norms can influence behaviors and outcomes. The workshop aimed to help physicians understand these concepts, recognize gender biases, and implement gender-sensitive approaches to improve health equity.






![EDUCATION AND RESEARCH
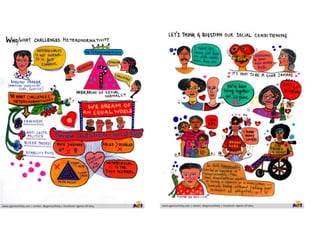
- Do we have enough information and is there
enough research on how to differentially
diagnose, treat and manage conditions among
men and women?
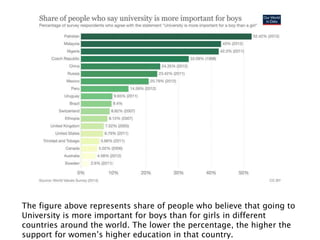
The inequality in how women are treated for pain in Europe
How’s the situation in India? [For example, routine episiotomies
during childbirth without anaesthesia]](https://image.slidesharecdn.com/genderworkshopforphysicians-240112064113-831d5fd8/85/Gender-workshop-for-physicians-pptx-28-320.jpg)