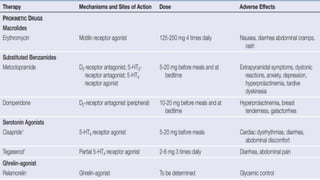
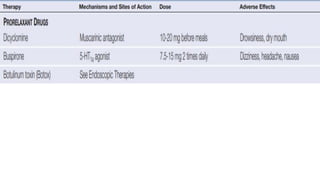
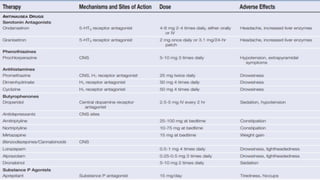
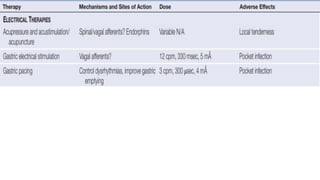
The document provides a comprehensive overview of gastric disorders, covering congenital disorders, mechanical issues, inflammation, and neoplasms. It discusses the anatomy and physiology of the stomach, gastric neuromuscular function, and various gastrointestinal disorders associated with gastric dysfunction. Additionally, it elaborates on diagnostic approaches and treatment options for conditions like gastroparesis and peptic ulcer disease.











![Pud Gastritis Lecture[1]](https://cdn.slidesharecdn.com/ss_thumbnails/pudgastritislecture1-1232045267191333-1-thumbnail.jpg?width=640&height=640&fit=bounds)











![Stomach by kp [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/stomachbykpautosaved-140422141057-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

![3.Presentation Gastric Secretion[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/3-260129133841-1fd04283-thumbnail.jpg?width=640&height=640&fit=bounds)





























