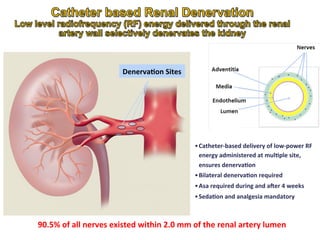
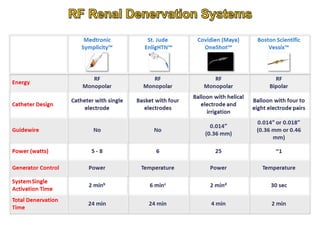
1. Renal denervation is a catheter-based procedure that uses radiofrequency energy to ablate renal nerves and lower blood pressure in patients with resistant hypertension.
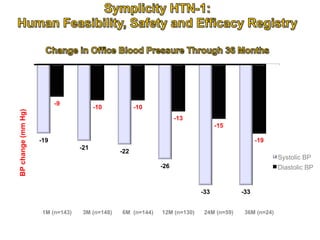
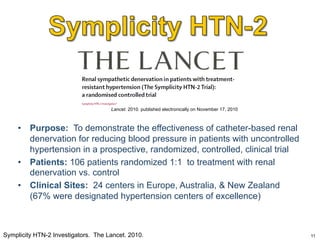
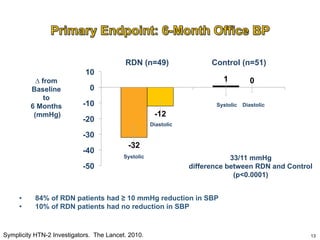
2. A randomized controlled trial found that renal denervation produced significant reductions in both systolic and diastolic blood pressure compared to a control group at 6 months.
3. Potential benefits of renal denervation beyond blood pressure lowering include reduced left ventricular mass, improved glucose metabolism, and fewer episodes of atrial fibrillation. However, long-term outcomes require further study.




















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)











