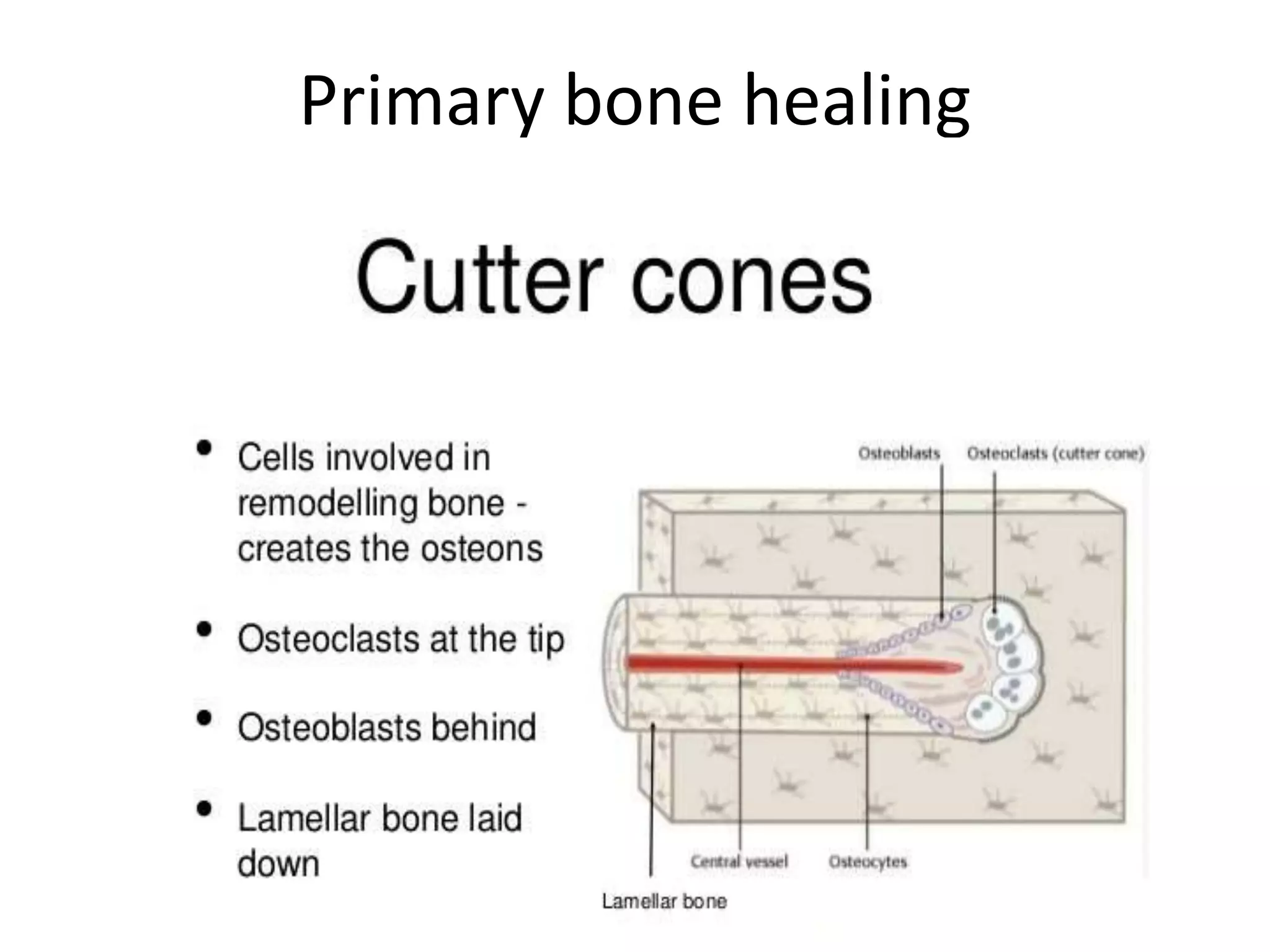
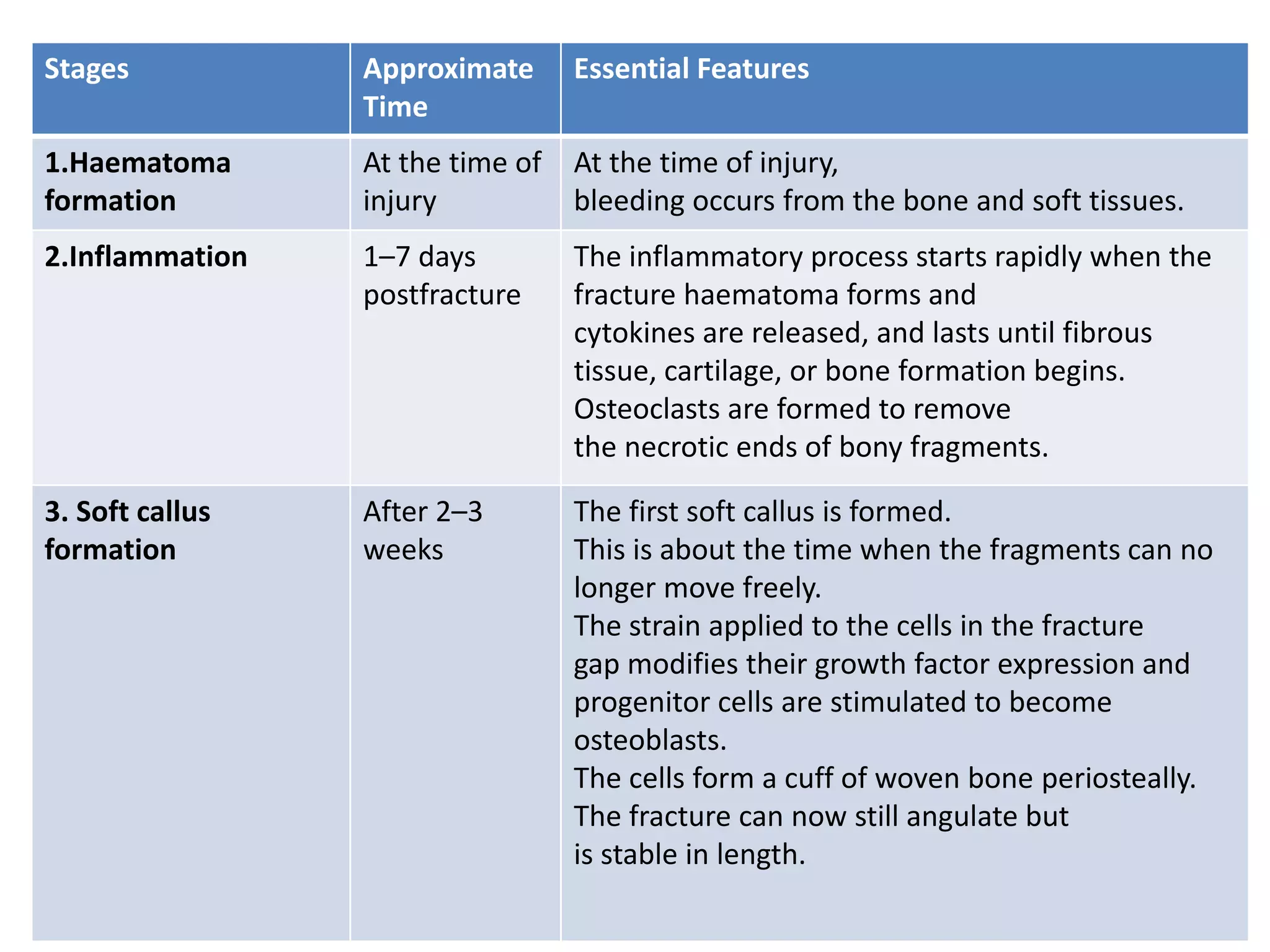
Bone healing occurs through either primary or secondary healing processes. Primary healing involves direct bone formation without callus and occurs under conditions of absolute stability. Secondary healing involves indirect bone formation with callus and occurs when there is some interfragmentary motion providing relative stability. It proceeds in five stages over 3-4 months: hematoma formation, inflammation, soft callus formation, hard callus formation, and remodeling. Complications can include delayed union if healing is slowed, malunion if fragments heal in a misaligned position, or non-union if no healing occurs over an extended period.



































































![2 FRACTURE HEALING reloaded [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/2fracturehealingreloadedautosaved-250810162739-94b56093-thumbnail.jpg?width=640&height=640&fit=bounds)





















