



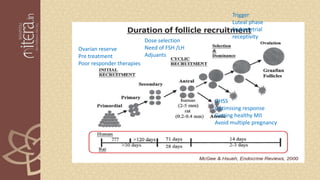
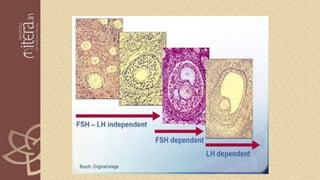

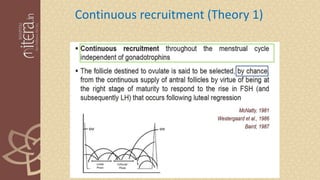
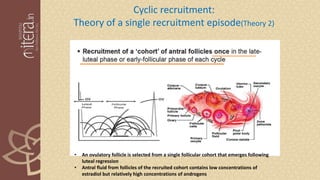
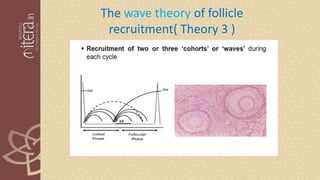
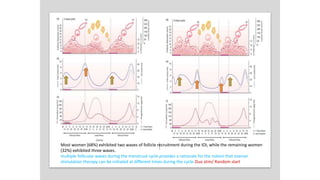
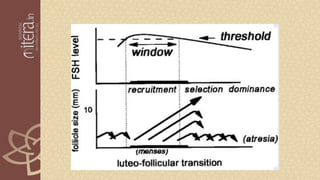
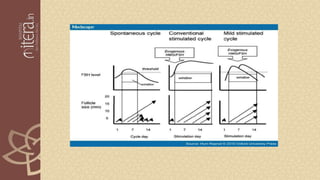
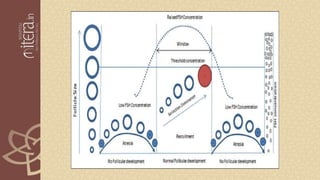
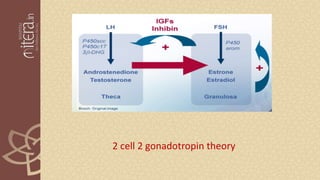


The document discusses the physiology of ovulation induction and ovarian folliculogenesis, emphasizing historical perspectives and hormonal regulation. It details the mechanisms behind follicle recruitment, selection, and dominance, exploring various theories related to follicular dynamics and the importance of FSH and LH in these processes. Ultimately, it highlights the relevance of understanding physiological concepts in developing effective ovulation induction protocols in reproductive medicine.











































































